Ear Tubes
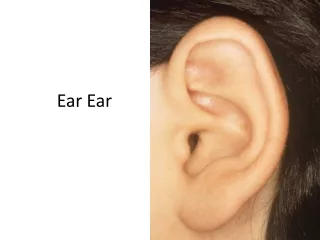
Ear Tubes. The Ear. AOM vs. OME. Otitis Media with Effusion Fluid behind TM May result from AOM Less sever complications Hearing loss Scarring/atrophy of TM Tympanosclerosis Do not treat with antibiotics Ear tubes if persistent or chronic. Acute Otitis Media Pus behind TM

Ear Tubes
E N D
Presentation Transcript
AOM vs. OME • Otitis Media with Effusion • Fluid behind TM • May result from AOM • Less sever complications • Hearing loss • Scarring/atrophy of TM • Tympanosclerosis • Do not treat with antibiotics • Ear tubes if persistent or chronic • Acute Otitis Media • Pus behind TM • Acute infection • Multiple severe complicaitons • Mastoiditis • Meningitis • Brain abscess • Facial paralysis • Treat with antibiotics • Ear tubes if recurrent
Types of TM Findings Serous otitis media Normal TM Mucoid Otitis Media Acute Otitis Media
Acute Otitis Media Peak incidence AOM is between 6 and 18 months AOM affects 40%-50% of children by age 1 By age 3 years majority (>80%) of children have had 1 episode of AOM ~ 40% of pediatric office visits in first 5 years related to otitis media ~5-10% of well visits associated with diagnosis of OME
Acute Otitis Media Diagnosis Certain diagnosis of AOM meets all 3 of the criteria: Presence of Purulent Middle Ear Effusion Rapid onset Signs and symptoms of middle-ear inflammation Otalgia No pain with pulling of ear TMJ pain Difficulty sleeping due to pain
Acute Otitis Media Diagnosis Pulling at the Ears (not reliable): Zero percent of children with ear pulling as the primary sign had an ear infection Ear pulling + fever: only 15% had ear infections Why do kids pull their ears? Itching Teething Exploration Comfort Habit Pain • Is ear pulling associated with ear infection. • Baker RB. Pediatrics. 1992 Dec;90(6):1006-7 • Diagnostic accuracy and the observation option in • acute otitis media: the Capital Region Otitis Project. • Gurnaney H, Spor D, Johnson DG, Propp R. • Int J Pediatr Otorhinolaryngol. 2004 Oct;68(10):1315-25
Acute Otitis Media Diagnosis Presence of Purulent Middle Ear Effusion Exam- Unobstructed ear canal and good light! Bulging of the tympanic membrane Limited or absent mobility of the tympanic membrane Pneumotoscopy Tympanometry Air-fluid level behind the tympanic membrane Otorrhea (purulent)
Misdiagnosis of Acute OM Over-reliance on history TM color does not predict AOME-crying makes most tympanic membranes red Failure to evaluate tympanic membrane mobility (pneumatic otoscopy) Poor light from otoscope (bulb & battery) Failure to remove cerumen Inappropriate sized speculum Lack of experience
Acute Otitis Media Improving diagnostic accuracy: Pneumatic otoscopy Otomicroscopy
Acute Otitis Media Treatment Why do we treat AOM? Quality of Life Suppurative Complications Once treated, when do we follow-up? If asymptomatic, follow-up is to ensure resolution of fluid This process can take up to 3 months (74%) • Intracranial Complications: • Meningitis • Extradural abscess • Subdural empyema • Lateral sinus thrombosis • Brain abscess • Otitic hydrocephalus • Extracranial Complications: • Mastoiditis • Petrositis • Facial Paralysis • Perforation of the TM • Hearing loss • CHL • SNHL • Labyrinthitis
Acute Mastoiditis May or may not be associated with subperiosteal abscess Protrusion of the auricle may be secondary to osteitis of the mastoid cortex without erosion/ abscess
Tubes for Acute Otitis Media Recalcitrant- persistent acute infection despite antibiotics Recurrent 3/6 or 4/12 or 6/12 total duration Parental concern Day care At risk populations Time of year Adenoidectomy if recurrent bacterial URI/sinusitis Complications
AOM vs. OME • Acute Otitis Media • Pus behind TM • Acute infection • Multiple severe complicaitons • Mastoiditis • Meningitis • Brain abscess • Facial paralysis • Treat with antibiotics • Ear tubes if recurrent • Otitis Media with Effusion • Fluid behind TM • May result from AOM • Less sever complications • Hearing loss • Scarring/atrophy of TM • Tympanosclerosis • Do not treat with antibiotics • Ear tubes if persistent or chronic
Otitis Media with Effusion Tympanic membrane characteristics Translucent or opaque Gray, white, yellow, or pink color Neutral or retracted position Reduced mobility, responds to negative pressure on pneumatic otoscopy Effusion present
Otitis Media with Effusion Treatment Intervention based on severity of hearing loss, child’s developmental status, parent preference Aggressive management of “at-risk” population Watchful waiting for at least 3 months in “non at-risk” population “Paradise Tube Article” studies only healthy, non at-risk children Nasal steroids may help Nasal decongestants/antihistamines of no proven use Antimicrobials/steroids not indicated Paradise JL., et al: Tympanostomy Tubes and Developmental Outcomes at 9 to 11 Years of Age N Engl J Med. 363 (3):248-261, 2007.
Otitis Media with Effusion Treatment Audiogram if fluid > 3 months If normal hearing periodic re-evaluation until clear; more aggressive intervention if hearing loss, behavior problems or TM changes Surgery- Tubes with or without adenoids Tubes initially only Adenoidectomy if nasal obstruction or infection problems or if past hx of tubes Repeat surgery--adenoidectomy +/-tubes
AOM vs. OME • Acute Otitis Media • Pus behind TM • Acute infection • Multiple severe complicaitons • Mastoiditis • Meningitis • Brain abscess • Facial paralysis • Treat with antibiotics • Ear tubes if recurrent • Otitis Media with Effusion • Fluid behind TM • May result from AOM • Less sever complications • Hearing loss • Scarring/atrophy of TM • Tympanosclerosis • Do not treat with antibiotics • Ear tubes if persistent or chronic
Ear Tube Placement • Radial incision • Anterior/inferior quadrant
Post-Operative Care • Ear drops for 2-7 days • If fluid present • Floxin, Ciprodex, Saline • Never “Cortisporin” or gentamicin • See at 2-4 weeks • Audiometry • Clean tube is occluded • Replace tube if unsuccessful • See every 6-12 months until extrusion/healing
Complications • Early Complications • Tube occlusion • Extrusion • Otorrhea • Impaction into middle ear • Hearing loss • Delayed Complications • Otorrhea • Perforation • Retention • Myringosclerosis • TM atrophy • Hearing loss • Tympanosclerosis • Cholesteatoma
Questions? Thank You!