Download
1 / 38
380 likes | 472 Views
MANAGEMENT OF CARDIAC SURGICAL PATIENTS RECEIVING PLATELET INHIBITORS. Jerrold H. Levy, MD Professor of Anesthesiology Emory University School of Medicine Director of Cardiothoracic Anesthesiology Emory Healthcare Atlanta, Georgia. Events Leading to Thrombus Formation. Adhesion.

E N D
MANAGEMENT OF CARDIAC SURGICAL PATIENTS RECEIVING PLATELET INHIBITORS Jerrold H. Levy, MD Professor of Anesthesiology Emory University School of Medicine Director of Cardiothoracic Anesthesiology Emory Healthcare Atlanta, Georgia
Events Leading to Thrombus Formation Adhesion Activation Aggregation
Gp IIb/IIIa ANTAGONISTS • Platelet Gp IIb/IIIa receptors play a pivotal role in platelet-mediated thrombus formation, binding to binds to fibrinogen and vWF • IIb/IIIa antagonists differ in receptor affinity, reversibility, and specificity
PLATELET INHIBITORS • ASA • Clopidogrel (Plavix), Ticlid • Aggrastat (tirofiban) • ReoPro (abciximab) • Integrilin (eptifibatide)
Platelet Activation Pathways Collagen Thrombin Epinephrine ADP Arachidonic acid TxA2 GP IIb/IIIa
GP IIb/IIIa antagonist Inhibition of platelet aggregation GP IIb/IIIa receptors occupied by antagonists Agonist ADP, thrombin, collagen Resting platelet GP IIb/IIIa receptors in unreceptive state Fibrinogen Aggregating platelets
Tirofiban (Aggrastat) • Nonpeptide • KD 15 nmol/L • Indication: acute coronary syndrome
Eptifbatide (Integrelin) • Cyclic peptide • KD 120 nmol/L • Acute coronary syndrome
Abciximab (ReoPro) • Human/murine chimeric monoclonal antibody Fab • KD 5 nmol/L • Indication: PCI
PLATELET DYSFUNCTION DURING CPB • Hemodilution • Contact activation • Shear stresses • Hypothermia • Intrinsic/extrinsic defects • Anticoagulation/reversal
PLATELET FUNCTION AGGREGATION • IIb/IIIa - fibrinogen interaction • Key step for hemostasis, part of final common pathway • Therapeutic target of inhibitors
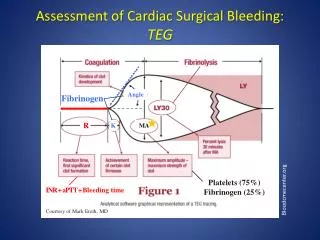
PLATELET FUNCTION EVALUATION • Platelet count • Bleeding time • Aggregation • TEG/SonoClot • Platelet function assays • Accumetrics
Accumetrics’ Ultegra System Step 1 Step 2 Step 3 Insert Cartridge Insert whole blood sample Read result in 60 seconds
Correlation of Platelet Aggregation and Accumetrics RPFA y = 0.9874x - 0.4028 = 0.988 10 20 30 40 50 60 70 80 90 100 Mean and S.D. of 6 Donors 100 90 80 70 Aggregometry (%) 60 50 40 r2 30 20 10 0 Accumetrics RPFA (%)
Gammie: Abciximab and excessive bleeding in patients undergoing emergency cardiac operations. Ann Thor Surg 65:465-9, 1998 • 11 pts req emerg CABG, operated on <12 hr after abciximab (n = 6), or late >12 hr after abciximab (n = 5) • Postop drainage (1,300 vs 400 mL) • Tx pRBC (6 versus 0 U; p = 0.02), • Platelets transfused (20 versus 0 packs) • Max ACT (800 vs 528 sec; p = 0.01)
Methods (EPILOG and EPISTENT Trials) • Patients undergoing CABG during index hospitalization • Data from both CRF andretrospective data collection at sites • Pooling of all abciximab tx groups and of all placebo groups in 39 sites • Most patients were unblinded undergoing CABG
5 5 Placebo 4 4 3.8 3.8 3 3 2 2 1.5 1.5 1.5 1.5 1 1 1.1 1.1 0 0 EPILOG EPISTENT EPILOG EPISTENT Patients requiring CABG following Abciximab % Abciximab
Pre-Operative Anticoagulation Placebo Abciximab (n = 37) (n = 41) Total heparin (U) 12,000 6500 (8600 - 12,000) (5900 - 6500) Total heparin (U/kg) 146 77 (100 - 195) (70 - 106)
Anticoagulation and Surgery Placebo Abciximab (n = 34) (n = 40) OR heparin load 26,500 27,000 (18,000 - 30,000) (10,000 - 30,000) OR heparin on pump 10,000 7000 (5000 - 15,000) (5000 - 10,000) OR heparin total 35,000 31,000 (26,000 - 51,000) (13,800 - 40,000)
Operative ACTs and Abciximab Placebo Abciximab (n = 32) (n = 36) Pre-op ACT 207 166 (152 - 266) (154 - 223) First ACT on pump 597 646 (478 - 751) (530 - 864) Highest ACT 600 711 (568 - 786) (580 - 999)
Operative Data and Abciximab Placebo Abciximab (n = 36) (n = 42) Total pump time (hr) 1.3 1.4 (0.8 - 1.7) (0.8 - 1.8) Total OR time (hr) 3.4 4.5 (3.0 - 5.1) (3.5 - 5.3) Off pump to close (hr) 0.9 0.9 (0.5 - 1.1) (0.6 - 1.4)
Hemostatic Agents and Abciximab Placebo Abciximab (n = 37) (n = 43) Cryoprecipitate 22% 12% Autotransfusion 57% 61% Auto-tx volume 1090 ml 1038 ml Aminocaproic acid 32% 44% Aprotinin 8% 2% Desmopressin 3% 5% Re-exploration 1 5 Diffuse oozing 1 2 Other bleeding 0 3
¨ Chest tube drainage and Abciximab 4000 4000 Drains (ml) 3000 3000 2000 2000 ¨ 1000 1000 0 0 Placebo Abciximab Placebo Abciximab
Time £ 12 hr Time > 12 hr Abciximab and Bleeding Time to Surgery Placebo Abciximab Placebo Abciximab RBC Tx 78% 87% 69% 64% Plt Tx 44% 67% 13% 42% Major bleed 89% 96% 63% 75% Drain Blood Loss (ml) 730 870 1057 700 Hgb decrease (mg/dl) 7.8 9.4 7.3 7.1 Death or MI 72% 46% 17% 8%
Abciximab and CABG • Increased bleeding risk with urgent CABG • Abciximab therapy associated with minimal increase in blood loss with urgent CABG with conventional heparin dosing and platelet Tx transfusions • Patients requiring surgery in first 12 hours are at highest risk
TICLOPIDINE AND CLOPIDOGREL • Antiplatelet agents are used to treat, prevent arterial thrombosis. • Thienopyridine derivatives,inactive in vitro, requiring metabolism to achieve in vivo activity. • Inhibit binding of ADP to platelet receptor, inhibiting fibrinogen binding to the IIb/IIIa complex.
TICOLPIDINE/CLOPIDOGREL • In CAD stenting, ticlopidine reduces risk for subacute stent thrombosis • Clopidogrel reduces ischemic events with recent MI, stroke, or PVD • Clopidogrel + aspirin in stenting, is rapidly growing, given before stenting procedure • Bleeding variability for cardiac surgery relates to the duration of therapy
TICOLPIDINE and CABGAnesth Analg 1999;88:SCA 105 • 96/1166 CABG pts receiving ticlopidine • 83% of ticlop pt also on ASA, 28% ticlop pt were urgent vs 9% • Blood loss >1500 ml/24 hr more frequent in ticlop (14% vs 5%) • 62% ticlop pts received allogneic blood vs 45% • pRBC Tx 2 units vs 0 • Post op CT drain >30% in ticlop .
HEMOSTATIC GOALS FOR CARDIAC SURGERY • Prevent clotting for cannulation and initiation of extracorporeal circulation • Reverse anticoagulation in a safe and complete manner. • Prevent the inflammatory effects of CPB and contact activation
FACTORS AFFECTING ACT • Factor deficiency: fibrinogen, XII, VIII • Contact activation inhibitors: aprotinin • Warfarin therapy • Heparin therapy • Hypothermia • Thrombocytopenia/cytosis • Platelet inhibitors
RECOMMENDATIONS FOR MANAGING PATIENTS RECEIVING ANTIPLATELET AGENTS AND REQUIRING CARDIAC SURGERY:
SAFETY Based on the data in press and published, urgent cardiac surgery can be safely performed on patients who have received abciximab or one of the other GpIIb/IIIa receptor inhibitors.
BLEEDING Although the relative risk of abciximab-related bleeding may be increased within 12 hrs, this should not preclude urgent CABG. Platelets may be needed, and should be available when operating on abciximab-tx pts.
HEPARIN DOSING There are no data to support reductions in heparin dosing during CPB and for cardiac surgery. Therefore, standard-loading doses should be considered and additional heparin doses, based on time and duration of bypass or on actual heparin levels, should be maintained.
PLATELETS Platelets can be transfused to correct the bleeding defects associated with abciximab use. However, patients should not receive routine platelet transfusion prior to surgery and CPB. Rather, platelets should be administered after heparin reversal by protamine and after CPB.
SUMMARY: PLATELET INHIBITORS AND CARDIAC SURGERY • Do not transfuse with platelets before CPB • Normal heparin doses • Platelet transfusions when needed after CPB