Download
1 / 17
171 likes | 283 Views
Taking Aim at Mortality Scores. Clinical Documentation Improvement Nurses Effecting a Positive Change Suzanne Schultz, RN, CCDS Claudia Baker RN, CCDS. FLETCHER ALLEN HEALTH CARE. Vermont’s academic medical center in alliance with the University of Vermont in Burlington, Vermont 562 beds

E N D
Taking Aim at Mortality Scores Clinical Documentation Improvement Nurses Effecting a Positive Change Suzanne Schultz, RN, CCDS Claudia Baker RN, CCDS
FLETCHER ALLEN HEALTH CARE • Vermont’s academic medical center in alliance with the University of Vermont in Burlington, Vermont • 562 beds • Level 1 Trauma Center, Level 111 NICU, Children’s Hospital. • Approximately 6,500 employees • Staff of 900 physicians, 250 community physicians, 230 residents, 60 fellows • Approximately 200 NP’s and PA’s collectively • 5 CDI Registered Nurses
Objectives • Clinical Documentation Improvement Program at FA • CDI: Background and Process • University Health Care Consortium: Partner in Improvement • Why is Mortality Important? • UHC Mortality Ratio • Mortality Case Study • Closing statements
Goals of Clinical Documentation Improvement • Medical records are the foundation of any medical institution because the record is a representation of the patients, who are the very reason why we exist. • Documentation that captures a patient’s true co-morbidities, severity of illness and risk of mortality is essential. • The goal of CDI is high quality documentation that is accurate, concise, clear, complete, reliable and in accordance with the law.
CDI Program at Fletcher Allen Initiated in October 2009 4 RN’s and one Director Medical Director 3M consultants for 6 months, dedicated software 8 Inpatient Coders and Nurse Coding Supervisor as Liaison.
FLETCHER ALLEN CDI • Focused Medical Record Review • Query and Documentation Clarification: Standardized process based on FA CDI policy, which abides by the guidelines of AHIMA. • CDI Education for Providers: Formal presentations to provider groups that are tailored to their individual needs which enhances relevance. • Rounding with specific resident teams to provide on the spot education and support.
Documentation Clarification • Lack of Clarity • Lack of Specificity • Conflicts with other documentation • Please provide a diagnosis that corresponds with the lab value of Na 123 documented in your progress note on Oct 24 in Mrs. Jones’ medical record. • Dear Provider, Please spell out what you mean by AKI in your note on Mr. Smith on Oct. 24.
Work Flow of CDI - Clarification Process 1. Provider documents initial assessment. 2. CDI reviews record. 3. Documentation is accurate /complete. Next review date assigned. 4. If documentation requires clarification/specificity? 5. Query initiated and provider contacted. 6. CDI re-reviews record, documentation complete and accurate. Next review date assigned. 7. Documentation is not complete- Patient discharged. Attending is contacted about clarification. 8. Still not complete, CDI Medical Director Review.
Mortality Data and the University Healthcare Consortium • UHC is an alliance of the nations leading nonprofit academic medical centers totaling 114 and 255 total affiliated hospitals. • Comparing Fletcher Allen to other academic medical centers is a more appropriate comparison than a broad national comparison that doesn't reflect a similar patient population. • The Expected Mortality is a calculated measure developed by UHC and is based on “risk adjustment” information about FA patients. Risk models are periodically recalibrated due to reductions in LOS and mortality rates.
Definition of Terms • Severity of illness (SOI) is defined as the extent of organ system derangement or the physiologic decompensation of a patient. • Risk of mortality (ROM) provides a medical classification to estimate the likelihood of in-hospital death for a patient. The ROM class is used for the evaluation of patient mortality. • Mortality Rate is total number of deaths. • Observed to Expected Mortality(O:E) ratio is defined as the total number of deaths compared to the total number of expected deaths based on risk adjustments. Risk adjustments include patient-related age, gender, or pre-existing conditions. • Diagnosis-related group (DRG) is a system that classifies hospital cases. DRG’s are used to determine how much CMS pays a hospital for services.
Why are Mortality Scores Important • Hospital Report Cards are on the web and include mortality data. • Mortality rates are considered by the JCHO to be one of the important indicators of quality. • CMS, in the interest of promoting high quality , patient –centered care and accountability, reports 30 day mortality measures to the public. • Mortality rates for Pneumonia, Heart Attack, and Congestive Heart Failure are viewed as indicators of overall performance for a hospital. • CMS is collecting data now to establish Value Based Purchasing (VBP) benchmarks.
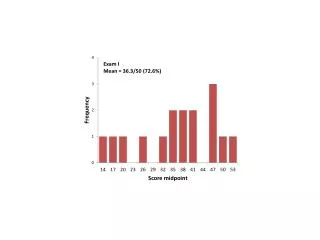
Mortality O:E Ratio Confidentiality Notice:This message, and any attachments, may contain information that is confidential, privileged, and/or protected from disclosure under state and federal laws that deal with the privacy and security of medical information, including confidential peer review information under 26 V.S.A. Sections 1441-1443.
Together and as a Team: Getting Closer to the Target Measurable Improvement in Mortality Scores Realized • Our Quality Improvement Consultant from the Jeffords Institute for Quality, Pat Bouchard, HIM Coding Supervisor Martha Sheehey and the CDI nurses identified opportunities to take the mortality review process to another level. • Based on a quality of care metric to drive improvements. • February 2011 was the lowest monthly O:E value for mortality to that date and was the 4th consecutive month demonstrating a decline. • This was significant.
Mortality Case Study • 75 yo male, VNA called FA ED, patient not doing well at home. Transported via amb w/ 100% NRB, O2 sat 81%, 89% in ED. B/P 92/48-81/38, resp 28-30, temp 101.2. PMH significant for COPD, CHF, HTN, CAD, CKD, HLP. In ED, desaturated with venti-mask O2 after nebulizer. CXR reveals bil infiltrates/edema. BIPAP applied. IV hydration w/ B/P responding. Labs Na 148, K+ 5.6, Creat 2.30. Admitted MICU w/ appropriate protocols. BLD draw in 4 hours. Records show last ECHO 30% EF. CODE STATUS: DNR/DNI. Bipap OK. Family to come in.
In Closing • Thank you for your time and attention. • Thanks you to our Team Partners: Quality Consultant Pat Bouchard; Martha Sheehey, Coding Liaison and the HIM Staff; Dr. Norm Ward, Medical Director for CDIP; FA Medical Staff and Residents, and the Nursing Staff at FA. • Contact: Suzanne Schultz by e-mail at suzanne.schultz@vtmednet.org • Claudia Baker by e-mail at claudia.baker@vtmednet.org