Download
1 / 35
450 likes | 1.58k Views
Effect of chest physiotherapy on respiratory mechanics. By Dr Sahar Elkaradawy Professor in Anaesthesia and Pain Management. Objectives. Basic mechanism of breathing. Effect of sedation and mechanical ventilation on respiratory mechanics.

E N D
Effect of chest physiotherapy on respiratory mechanics. By Dr SaharElkaradawy Professor in Anaesthesia and Pain Management
Objectives • Basic mechanism of breathing. • Effect of sedation and mechanical ventilation on respiratory mechanics. • Role of physiotherapy during mechanical ventilation.
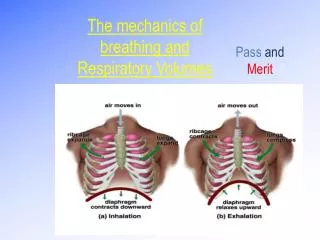
Basic mechanism of breathing • Expansion of the lungs ( during inspiration) is carried out by skeletal muscle contraction, but there is no direct connection between the respiratory muscles and the lungs
Pleural space and pressure • Between the lungs and the chest wall, there is a space: the pleural cavity. The mechanical behaviour of this airtight space follows Boyle's law, meaning that its pressure is inversely proportional to its volume. • Both the lungs and the chest wall have elastic properties. The chest wall has tendency to expand, while the lungs tends to collapse.
Pleural space and pressure • In this way, the movements of either the lungs or chest wall change the volume of the pleural cavity and, create negative intrapleural pressure.
Spontaneous ventilation • Trans-pulmonary pressure= intra alveolar p - intrapleural p. • Intra-alveolar p in resting position is zero. -1 or +1 in inspiration and expiration • Intra- pleural p is always negative. During inspiration, it reaches -6
Spontaneous ventilation • During inspiration, diaphragm and intercostal muscle activate to expand lung and decrease intrapleural P (-7). As a result, intra- alveolar P decreases and gas flows. At end of inspiration airflow ceases and intra- alveolar P becomes zero. • During expiration, diaphragm relaxes, intra pleural P becomes less (-5) and elastic recoil of lung makes lung to collapse and gas flows out
Effect of anaesthesia and deep sedation in lung mechanics • ↓function residual capacity( FRC) • Lung atelectasis • retention of secretion • ↑degree of V/Q mismatching. So change in patient position in ICU and physiotherapy are of para- amount important to improve lung oxygenation.
ventilator associated pneumonia Intubation and mechanical ventilation may impair mucociliary clearance and lead to: sputum retention, airway occlusion, atelectasis, ventilator associated pneumonia (VAP).
Chest physiotherapy Chest physiotherapy is the term for a group of treatments designed to improve respiratory efficiency, promote expansion of the lungs, strengthen respiratory muscles, and eliminate secretions from the respiratory system.
Chest physiotherapy is the most important strategy for prevention and treatment chest problems in ICU. Physiotherapists provide various chest physiotherapy techniques such as suctioning, patient positioning, chest vibrations, chest percussions, various coughing techniques in combination or individually to prevent and treat pulmonary complications like VAP and atelectasis in the ICUs.
Why physiotherapy? Their role is very important to: • encourage weaning • enhance patient’ wellbeing • reduce ICU stay • decrease cost
There are several modes of chest physiotherapy maneuvers were used for the patients under mechanical ventilation
Manual hyperinflation • MH involves disconnecting the patient from the ventilator and inflating the lungs with a large tidal volume (Vt) via a manual resuscitator bag (2.0-L). • MH is used with the aim of preventing pulmonary collapse, reexpanding collapsed alveoli, improving oxygenation and lung compliance, and increasing movement of pulmonary secretions toward the central airways.
Manual hyperinflation • The technique is usually performed by delivering a slow deep inspiration ( 3–5 s), an inspiratory hold, and a quick release of the inflation bag to enhance expiratory flow rate • The MH procedure was carried out daily at the rate of 8–13 breaths/min for a period of 20 min. After MH, immediately chest vibrations were also employed
Manual hyperoxygenation • manual hyperoxygenation, is used to deliver high levels of oxygen, using a manual resuscitator bag, but with no attempt to increase Vt to the extent sought with MH. • Manual hyperoxygenation is usually performed before and between suction passes, with the specific intention of preventing suction-induced hypoxemia.
Chest vibrations • It was defined as the manual application of a fine oscillatory movement combined with compression to the patient’s chest wall which helps to loosen and mobilize the secretions was given prior to suctioning. • The patient was positioned in supine, and then randomly positioned either to right or left side lying in the bed.
The principal investigator placed her hands anteriorly and laterally on the patient’s chest with fingers placed in the inter-rib space, and then applied vibrations in the expiratory phase of breathing.
This technique was repeated twice in each of the three zones, i.e., upper zone, middle zone, and lower zone of the chest .
Chest Percussion • Chest percussion, also referred to as chest physiotherapy, is an airway clearance technique that involves clapping on the chest and/or back to help loosen thick secretions. Doing this makes mucus easier to expel, or cough up. • Chest percussion is often coupled with postural drainage and vibration, and can be performed using cupped hands.
Chest percussion works best after a bronchodilator treatment. This should be performed over the lung segment that is to be drained. Your hand should be NOT be flat, but cupped at all times, as if you were holding liquid in it.
The percussion technique should be vigorous and rhythmical, but it should not involve pain. If the patient does complain of pain, this means that your hand may not be cupped properly and needs to be softened or readjusted. When done properly, you should hear a hollow sound with each percussion.
It should be done over the ribs, with careful attention to avoiding percussing over the spine, breast, or lower back to prevent damage to internal organs. Percussion may, or may not, be accompanied by vibration.
Suctioning Duration of endotracheal suctioning was limited to 15 s. To standardize the suctioning procedure and to enhance aspiration of dry secretions in some patients, 1 mL of normal saline via the tracheal tube before MH was done. The suctioning session involved instillation of 1 mL of normal saline in the tracheal tube, followed by suctioning once every minute for 4 min.
The sizes of the suctioning catheters used were FG14, and FG16 .The suctioning device was inserted fully up to the carina and then withdrawn for 1 cm prior to the application of negative pressure. During suctioning, the specimen from the lower respiratory tract was collected in a sterile container after instillation of 1 mL of normal saline for culture and sensitivity testing.
Positioning At the end of the treatment session, i.e., after suctioning, the head end was arranged to be positioned at an angle of elevation in the range of 30-45° and this positioning was maintained for minimum of 30 min for improving the ventilation in all patients. The change of positioning from lying supine to lateral orientations by turning the patients was manually done by nursing staff once in every 2 h
Normal response to physiotherapy: • Increased volume of sputum secretions. • Changes in breath sounds. • Improved vital signs. • Improved chest x ray. • Increased oxygen in the blood as measured by arterial blood gas values. • Patient reports of eased breathing.
Risks of chest physiotherapy: • Oxygen deficiency if the head is kept lowered for drainage. • Increased intracranial pressure. • Temporary low blood pressure . • Bleeding in the lungs . • Pain or injury to the ribs, muscles, or spine. • Vomiting • Inhaling secretions into the lungs . • Heart irregularities
References • Paulev-Zubieta. Gas Exchange and Disorders In:Poul-Erik Paulev & Gustavo Zubieta-Calleja New Human Physiology | 2nd Edition 2004,Chapter 14. • West, J.B. Respiratory Physiology: The Essentials. 8th Ed . Williams & Wilkins, Baltimore. USA, 2008. • Kathy Stiller Physiotherapy in Intensive Care:Towards an Evidence-Based Practice. Chest May 17, 2000 • ,