Download
1 / 13
130 likes | 294 Views
Acute Adrenal Crisis Related to Exogenous Steroid Use and Surgical Stress. Kenny-Joe Wallen The University of Kansas. Life is full of Stress. Physical Mental Emotional Nutritional Chemical Traumatic Pyscho-spiritual. General Adaptation Syndrome. Stage 1- Alarm

E N D
Acute Adrenal Crisis Related to Exogenous Steroid Use and Surgical Stress Kenny-Joe Wallen The University of Kansas
Life is full of Stress • Physical • Mental • Emotional • Nutritional • Chemical • Traumatic • Pyscho-spiritual
General Adaptation Syndrome • Stage 1- Alarm • Fight or Flight Response- SNS activation • Hormone release and activation- Adrenalin • HPA axis- Cortisol • Stage 2- Resistances • PSNS activity returns • Glucose, Cortisol, and Adrenalin levels remain elevated in circulation • Stage 3- Exhaustion • If stressor continues beyond body’s capacity, organism exhausts resources and becomes susceptible to disease and death.
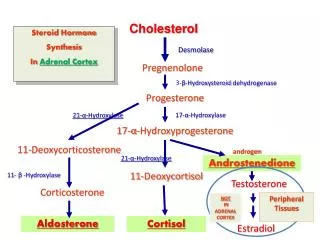
HPA Axis“The Stress Response” • Hypothalamus • Corticotropin-releasing hormone (CRH) • Pituitary Gland • Adrenocorticotropic (ACTH) • Adrenal gland • Glucocortacoids • Cortisol • Mineralocorticoids • Aldosterone • *HPA axis is regulated by a negative feedback mechanism
Adrenal Insufficiency • Primary- Destruction of all cortical zones • TB • Autoimmune • Congenital • Infection • AIDS most common cause • Malignancy • Trauma • Secondary • ACTH deficiency secondary to Hypothalamic or Pituitary dysfunction • HPA Suppression due to glucocorticoid therapy **Both forms will require supplemental steroids**
Corticosteroids • 1.2% of population > 20 yr (~2,513,259)/ over 20 years • 34 million prescriptions/ year • HPA suppression can occur after five daily doses of prednisone ≥ 20 mg and recovery of HPA function occurs gradually and can take up to 12 months • Adrenal gland atrophy and HPA suppression • Unable to respond to the stress of surgery
Surgery • One of the most potent activators of the HPA axis • Endotracheal Intubation • Reversal • Extubation • Negative feedback mechanism fails • ACTH and Cortisol • Cortisol • Normal secretion- 20-30 mg/day • During stress- as high as 200-500 mg/day
Surgery • Patients receiving chronic corticosteroid have atrophy of their adrenal gland and subsequent suppression of the HPA axis rendering them incapable of producing an adequate amount of endogenous glucocorticoids to meet the demands of the operative stress. These individuals will present with signs and symptoms of adrenal insufficiency
Adrenal Insufficiency • Signs and Symptoms • Hypoglycemia • Hypotension • Tachycardia • Tachypnea • Anorexia, weight loss • Nausea, Vomiting, Abd pain • Hypo NA • Hyper K • Acidosis • Mucosal and Skin pigmentation Δ • Muscle Weakness • Fever
Anesthetic Implications • Preoperatively • H&P • Disease Process • Medications • How long? Last dose? • Intraoperatively • Avoid Etomidate • Early recognition of S&S of adrenal crisis • Treatment • Rapid IV infusion with saline /c cardiac monitoring • Steroid replacement therapy “Stress dosing” • If hemodynamically unstable consider inotropic support
References Finnerty, C. C., Mabvuure, N. T., Ali, A., Kozar, R. A., & Herndon, D. N. (2013). The Surgically Induced Stress Response. Journal of Parental and Enteral Nutrition, 37 (Supplemental 1), 21S-29S. Fournier, D. J., & Galante, M. (1957) Operative and Postoperative Emergency Use of Hydrocortisone Derivatives and Corticotropin. Journal of California Medicine, 86 (6), 374-377. Jung, C., & Inder, W. J. (2008). Management of adrenal insufficiency during the stress of medical illness and surgery. Medical Journal of Australia, 188, 409-413. Karlet, M. C., & Fort, D. N. (2013) The Endocrine System and Anesthesia. In Nagelhout, J. P., & Plaus, K. (5th ed.), Nurse Anesthesia. St. Louis, MO: Saunders/Elsevier. Marik, P. E., & Varon, J. (2008). Requirement of Perioperative Stress Doses of Corticosteroids. Journal of Archive of Surgery, 143 (12), 1222-1226. Overman, R. A., Yeh, J. & Deal, C. L. (2013). Prevalence of oral glucocorticoid usage in the United States: A general population perspective. Arthritis Care & Research, 15 (3), 5-13. Schwartz, J. J., Akhtar, S., & Rosenbaum, S. H. (2013) Endocrine Function. In Barash, P. G., Cullen, B. F., Stoelting, R. K., Cahalan, M. K., Stock, M. c., & Ortega, R. (6th ed.), Clinical Anesthesia. Philadelphia, PA: Lippincott Williams & Wolters. Selye, H. (1978) The Stress of Life, revised edition. New York: McGraw-Hill. Tsigos, C. & Chrousos, G. P. (2002). Hypothalamic-pituitary-adrenal axis, neuroendocrine factors and stress. Journal of Psychosomatic Research, 53, 865-871.