Download
1 / 89
890 likes | 1.04k Views
DOUBLE TROUBLE (TB -HIV). Medical Grandrounds February17, 2010 Ledesma Hall Presenter: Kristine S de Luna Moderator: Dr. Maricel Gler. Objectives. 1. To present a case of a patient with AIDS who developed disseminated TB. 2. To discuss the pathophysiology of TB in AIDS.

E N D
DOUBLE TROUBLE(TB -HIV) Medical Grandrounds February17, 2010 Ledesma Hall Presenter: Kristine S de Luna Moderator: Dr. Maricel Gler
Objectives 1. To present a case of a patient with AIDS who developed disseminated TB. 2. To discuss the pathophysiology of TB in AIDS. 3. To discuss the challenges in the diagnosis of TB in AIDS. 4. To discuss the challenges in the treatment of TB in AIDS, as well as current guidelines in the management.
Identifying Data • R.A. • 51 years old, male • Single
Chief Complaint • Fever and cough
History of the Present Illness 1 month PTA cough; fever; weight loss (50%) 3 weeks PTA right upper quadrant abdominal pain nausea; appetite loss 2 weeks PTA GI consult, Impression: pancreatitis, liver abscess CT scan of the abdomen Meds: Cefixime, Metronidazole, pancreatin Infectious Diseases Specialist Referral
PLAIN ARTERIAL PORTAL VENOUS DELAYED
PLAIN ARTERIAL PORTAL VENOUS DELAYED
Prominent pancreatic head with moderate surrounding fat stranding and prominent lymph nodes. • Small pockets of air within the pancreatic head with a suspicious connection to the duodenum. Duodeno-pancreatic fistula has to be ruled out.
Mildly enhancing central focus with partially calcified wall in hepatic segment VII. • Ovoid focus in hepatic segment II, likely a hemangioma.
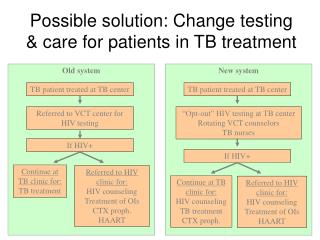
History of the Present Illness ADMISSION 5 days PTA Probable disseminated TB and immunocompromised state Few hrs PTA Persistence
Review of Systems no rashes no sore throat no difficulty in swallowing no chest pain no dysuria
Past Medical History (-) PTB gallbladder stones in 2005 post open cholecystectomy (-) blood transfusion
Personal Social History non-smoker Occasional alcoholic beverage drinker goes to the gym 3 times a week for 15 years Denies illicit drug use Admits to have unprotected sex with a male partner for the past 10 years Currently in a sexual relationship with a male
Family History (+) pulmonary tuberculosis- mother
Physical Examination BP: 100/60 CR: 110, reg RR: 22 T: 38.1 Height: 165.1 cm Weight: 65.2 kg BMI: 23.9 Pain Scale: 2/10 General Appearance: weak-looking, conscious, not in CP distress Skin: warm, no active dermatoses, (+) pallor HEENT: no nasaoaural discharge, no oral lesions, non-hyperemic posterior pharyngeal walls, tonsils not enlarged, 2 movable, non-tender, non-matted submandibular lymph nodes (approx 1 x 1 cm each) bilateral, midline trachea
Physical Examination Lungs: symmetric chest expansion, no retractions, equal vocal and tactile fremiti, resonant, clear breath sounds Heart: AB 5th LICS MCL, no heaves, no thrills, regularly regular rhythm, no murmurs Abdomen: flat, surgical scar RUQ, NABS, direct tenderness RUQ, no rebound tenderness, no masses, non-palpable liver edge, non-palpable spleen Genitourinary: no costovertebral angle tenderness Extremities: (-) edema, (-) cyanosis, pulses full and equal
AFB smear and TB PCR AFB smear result: Negative GeneXpert MTb/Rif result: MTB detected, No Rifampicin resistance
Initial Impression Pulmonary TB, Smear Negative To consider disseminated tuberculosis To consider immunocompromised state
DIFFERENTIAL DIAGNOSIS Source: Irwin, Richard MD & Mark Madison, MD. Diagnosis and Treatment of Cough. New England Journal of Medicine. Vol 343, No. 23 pg 1715 – 1721.
Course in the Ward Day 1: Admitted to isolation room.Referred to GI. The following were requested: CXR-PA , CBC, ESR, CRP Quantitative, CD4, blood CS at 2 sites, liver function test, amylase, lipase, prothrombin time. Meds: HRZE 4 tabs daily, pantoprazole 40 mg/IV once daily, vitamin B complex once daily, ocreotide drip x 24 hours, pancreatin 150 mg/tab 3 times a day .
AFB smear and TB PCR AFB smear result: Negative GeneXpert MTb/Rif result: MTB detected, No Rifampicin resistance
Course in the Ward Day 1: Admitted to isolation room.Referred to GI. The following were requested: CXR-PA , CBC, ESR, CRP Quantitative, CD4, blood CS at 2 sites, liver function test, amylase, lipase, prothrombin time. Meds: HRZE 4 tabs daily, pantoprazole 40 mg/IV once daily, vitamin B complex once daily, ocreotide drip x 24 hours, pancreatin 150 mg/tab 3 times a day .
Infiltrates in the right upper lobe, compatible with pulmonary tuberculosis of undetermined activity.
Course in the Ward Day 1:Admitted to isolation room.Referred to GI. The following were requested: CXR-PA , CBC, ESR, CRP Quantitative, CD4, blood CS at 2 sites, liver function test, amylase, lipase, prothrombin time. Meds: HRZE 4 tabs daily, pantoprazole 40 mg/IV once daily, vitamin B complex once daily, ocreotide drip x 24 hours, pancreatin 150 mg/tab 3 times a day .
Other Laboratory Tests CD4: 74/mm3 (500 to 1500/mm3) Blood CS:negative Prothrombin Time: normal
Course in the Ward Day 2: Febrile episodes. No pain. Abdomen: soft, non-tender. Ocreotide 100 mcg SC once a day. Day 3: For HBsAg, VDRL, anti-HCV, anti-HAV IgG, HIV viral load. Soft, low fat diet. May go home.
HBsAg: negative VDRL: negative Anti-HAV IgG:positive Anti-HCV: negative HIV VIRAL LOAD PCR:780, 000 copies/ml
HIV Screening, Agglutination (Dec 13, 2010):reactive to anti-HIV 1 • HIV Screening, EIA (Dec 14, 2010):reactive • Chemiluminescence Microparticle Immunoassay Test for HIV Ag/Ab, Western Blot (Dec 14, 2010):+ HIV Ab, bands present (gp 160, gp 120, p 66, p 51, gp 41, p 31, p 24)
Final Diagnosis • Disseminated Tuberculosis • Acquired Immune Deficiency Syndrome
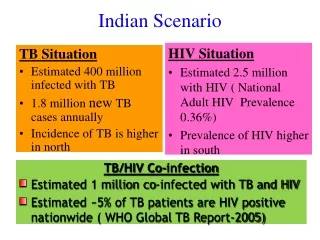
Epidemiology of TB The Philippines is the 9th among the the 22 high burden countries for TB
HIV Prevalence in the Philippines Department of Health – National Epidemiology Center November 2010
Department of Health – National Epidemiology Center November 2010
Mode of Transmission Types of Sexual Transmission
Dual infection HIV + TB