Download
1 / 20
200 likes | 415 Views
MLAB 1227: Coagulation Keri Brophy-Martinez. Coagulation Disorders: Secondary Hemostasis Part Two. Acquired Coagulation Disorders. Two or more factors generally affected, more complicated Bleeding from multiple sites More common than hereditary disorders Classification DIC

E N D
MLAB 1227: CoagulationKeri Brophy-Martinez Coagulation Disorders: Secondary Hemostasis Part Two
Acquired Coagulation Disorders • Two or more factors generally affected, more complicated • Bleeding from multiple sites • More common than hereditary disorders • Classification • DIC • Primary Fibrinogenolysis • Liver Disease • Vitamin K Deficiency • Acquired Pathologic Inhibitors
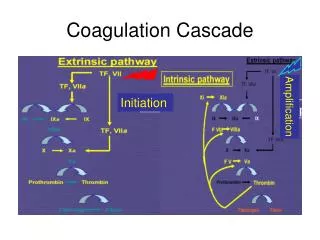
1. DIC: Disseminated Intravascular Coagulation • Consumption Coagulopathy • As fibrin is formed, clotting proteins and naturally occurring inhibitors and platelets are consumed faster than they are made • Thrombo-hemorrhagic disorder • Clotting and lysing occurring in blood vessel, at the same time • Life threatening • Bleeding is the most apparent characteristic • Initiating events are thrombotic, where material enters circulation • Occurs due to lack of the negative feedback mechanism • Affects young and elderly
DIC: Triggers • Obstetric – usually due to major tissue damage such as retained dead fetus, abruptio placentae, or placenta previa • Acute leukemias – Promyelocytic – increase number of granules released into circulation as cells break down • Intravascular hemolysis – ex: transfusion reaction • Massive trauma (especially crushing injuries), burns, surgical procedures • Heat stroke • Snake venoms • Septicemias and infections – viral, bacterial, rickettsial, fungal, protozoan (especially gram negative that release endotoxins) • Tumors – foreign tissues and cells • Prosthetic devices – heart valves, aortic balloon, peritoneal shunting • Vascular disease – damaged endothelial lining
DIC: How Does It Occur? • Step 1: Out of control clotting • Causes widespread fibrin deposits in vessels of tissues and organs • Subsequent event: Hemorrhage • Clotting proteins consumed at a high rate • Causes multiple factor deficiencies, especially fibrinogen group • Platelets caught in thrombi and removed
DIC: How Does It Occur? • Step 2: Triggers Fibrinolytic system to remove fibrin • Results in: • Circulating degradation products that interfere with platelet function & normal clot formation • Degradation of Factor V & VIII
DIC: How Does It Occur? • Step 3: Uncontrolled plasmin and thrombin enter circulation • Why? • Inhibitors such as AT have been depleted
DIC: How Does It Occur? • Step 4: Appearance of Symptoms • Bleeding from multiple sites • Petechiae • Purpura • Occlusions in organs • Oozing from arterial lines, venipuncture sites • Shock
Lab Features of DIC • Platelet count: decreased • (40-75 x 109/L) • PT: increased • PTT : increased • Fibrinogen: decreased • FDP /D-dimer: positive • **Most helpful in diagnosis • RBC fragments: present • AT : decreased
DIC • Treatment • Goal is to treat the underlying condition • Remove the triggering process – treat with antibiotics, antineoplasms, remove dead tissue, treat the diseases or conditions • Heparin – to prevent or limit further coagulation • Replace factors, platelets = give FFP
2. Primary Fibrinogenolysis • Similar to DIC • Plasminogen is inappropriately activated to plasmin • Plasmin circulates overwhelming the antiplasmin inhibitors and degrading fibrinogen and factors V,VIII, XIII • No thrombin is generated • Liver disease is a common trigger
3. Liver Disease • Affects all proteins made in the liver that function in fibrin formation, fibrinolysis and inhibition. • Patients show minimal bleeding, except in severe cases • Lab features • Increased • PT,PTT • Decreased • Platelets
4. Vitamin K Deficiency • Liver cells able to make precursor protein but the calcium binding site is nonfunctional • Causes • Malabsorptive syndromes • Sprue • Obstruction in biliary tract • Antibiotic therapy • Kills off normal flora in gut which made vitamin K
5. Acquired Pathologic Inhibitors • Develop in patients with certain disease states and others with no underlying conditions • Circulating anticoagulants which may develop against any clotting factor • Classed as immunoglobulins • Either IgG or IgM • Can be alloantibodies or autoantibodies • Not normally synthesized by the body, bind with the factors making them unavailable for use in the cascade
Types of Inhibitors • Directed towards a single coagulation factor • Seen in patients with inherited factor deficiencies that have had replacement therapy for bleeding complications • Less commonly seen in healthy people and those taking certain drugs • Rare, except Factor VIII & IX • How do we find them? • Interfere with clotting factor activity • PTT prolonged, other tests normal • Mixing study: test will still be prolonged
Types of Inhibitors • Lupus Inhibitor/Anticoagulant • Seen in patients with autoimmune diseases, drug reactions, but also in normal patients • Autoantibodiesinterfere with phospholipid-dependent reagents used in PTT tests • Patients have no bleeding problems (though some have an increase risk of thrombosis) • In vitro, any coag test using a phospholipid reagent will be falsely prolonged (PT, PTT) • Coag studies must be performed using reagents that do not contain phospholipids
References • McKenzie, Shirlyn B., and J. Lynne. Williams. "Chapter 32." Clinical Laboratory Hematology. Boston: Pearson, 2010. Print.