Download
1 / 52
1.05k likes | 6.18k Views
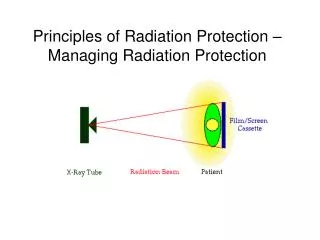
Introduction to Radiation Protection. Effective Radiation Protection. Radiation protection can be defined as effective measures employed by radiation workers to safeguard patients, personnel, and the general public from unnecessary exposure of ionizing radiation.

E N D
Effective Radiation Protection • Radiation protection can be defined as effective measures employed by radiation workers to safeguard patients, personnel, and the general public from unnecessary exposure of ionizing radiation. • That is why facilities should establish a radiation safety program. • It is important to ensure radiation safety during all medical radiation procedure.
Biologic Effects • The need for safety against significant and continuing radiation exposure is based on evidence of harmful biologic effects. • This can be applied to: the radiation worker, patient, or to the general public. • This biological effects depend on the radiation exposure or dose. Generally, exposure to these kinds of radiation would be very harmful to human beings. The effects could be either short-term or long-term.
Benefits Vs. Risk • Radiation exposure should always be kept as low as possible. • But, when illness and injury occurs or when a specific imaging procedure for health screening purposes is important, the patient can choose to assume the risk of the exposure to radiation to obtain an essential medical information.
Diagnostic Efficacy • Diagnostic efficacy is the degree to which the diagnostic study accurately reveals the presence or absence of a disease in the patient. • Efficacy is a vital part of radiation protection in the healing arts. • It provides the foundation for determining whether an imaging procedure or practice is acceptable.
Achievement of Diagnostic Efficacy • It is important for the referring physician to carry the responsibilities for determining the medical necessity for the patient. • After ordering an x-ray examination or procedure, the physician must accept basic responsibility to protect the patient from non-useful radiation exposure. • Its is also the radiographers responsibility for the patients well-being by providing quality imaging services.
Both the radiographer and the radiologist share in keeping the patient medical radiation exposure at the lowest level possible. • This way imaging professionals help ensure that both occupational and nonoccupational dose limits, that result in a negligible risk of bodily injury or genetic damage, will remain in well below maximum allowable.
ALARA • ALARA is an acronym for As Low As Reasonably Achievable. • The reason for this concept in radiologic practice is to keep radiation exposure and consequent dose to the lowest possible level. • For the radiographer and the radiologist the ALARA concept should serve as a guide for the selection of technical radiographic and fluoroscopic exposure factors for all patient imaging procedure.
Responsibility for Maintaining ALARA • It is the responsibility of the employer to provide the necessary resources and appropriate environment in which to execute an ALARA program. • To determine that proper lowered radiation exposure are being applied, management should perform periodic exposure audits. • Radiation workers with appropriate education and work experience must function with awareness of rules governing the work situations.
Patient Protection and Patient Education • Patients should always be aware of what type of procedures are being done, and what kind of cooperation is needed, but also they need to be informed from the radiologist of what is being done. • Through appropriate and effective communication, patients can be made to feel that they are active participants in their own health care.
Background Equivalent Radiation Time (BERT) • This method compares the amount of radiation received. • Radiographers can use this method to understand and reduce the fear and anxiety of the patient.
Types of Radiation • Radiation is defined as energy in transit from one location to another. • Radio waves, ,microwaves, visible light, and x-rays represent electromagnetic waves. • Electromagnetic waves are characterized by their wavelength.
Types of Radiation • The full range of frequencies and wavelengths of electromagnetic waves is known as Electromagnetic Spectrum. • Each frequency and within the spectrum has a characteristic wavelength and energy. • Electromagnetic spectrum can be divided into two parts: ionizing and nonionizing
Ionizing and Nonionizing • Only X-ray and gamma radiation are known as ionizing radiation. • Ultraviolet, visible light, infrared rays, microwaves, and radio waves are considered to be nonionizing radiation, because they do not have sufficient kinetic energy to eject electrons from the atom.
Ionizing and Nonionizing • Ionization is the foundation of the interactions of x-rays with human tissue. • The amount of energy transferred to the electrons by ionizing radiation is the basis of the concept of radiation dose.
Particulate Radiation • This radiation includes alpha particles, beta particles, neutrons, and protons. • These subatomic particles are ejected from atoms at very high speeds. • Particulate radiations vary in their ability to penetrate matter.
EQUIVALENT DOSE AND EFFECTIVE DOSE • Equivalent Dose (EqD)– A quantity that attempts to take into account the variation in biologic harm that is produced by different types of radiation. • Equivalent Dose (Eqd) enables the calculation of the Effective Dose (EfD) • Effective Dose (EfD) – A quantity that attempts to summarize the overall potential for biologic damage to a human due to exposure to ionizing radiation. • Effective dose takes into account organ weighting factors and represents the whole body dose that would give an equivalent biologic response. • EfD and EqD are both expressed in sieverts (Sv), used by the International System of Units (SI), or rem, which adopts the traditional measuring system
SOURCES OF RADIATION • Human beings are continuously exposed to sources of ionizing radiation • Ionizing radiation from environmental sources is called natural background radiation. • There are three types of natural background radiation: • Terrestrial Radiation • Cosmic Radiation • Internal Radiation
TERRESTRIAL RADIATION • Long-lived radioactive elements such as uranium-238, radium-226, and thorium-232 that emit ionizing radiations are present in variable quantities in the earth’s crust. • These elements are found in rocks, soil, the water we drink, the food we eat, and building materials. • Approximately 55% of the gross common exposure of human beings to natural background radiation comes from radon, contributing approximately 198mrem per year to the average American.
Cosmic Radiation • Cosmic rays are of extraterrestrial origin and result from nuclear interactions that have taken place in the sun and other stars. • Cosmic radiations consist predominantly of high-energy protons • The greatest intensity occurs at high altitudes, and the lowest intensity occurs at sea level. • The average U.S. inhabitant receives an average of 30mrem per year of extraterrestrial radiation.
INTERNAL RADIATION • The tissue of the body contain many naturally existing radionuclides that have been ingested in minute quantities from various foods or inhaled as particles in the air. • A radionuclide is an unstable nucleus that emits one or more forms of ionizing radiation to achieve greater stability. • Examples of internal radionuclides are: Potassium- 40, Carbon-14, Hydrogen-3 (Tritium), and Strontium-90 • An average individual receives approximately 67mrem per year from combined exposure to radiations from the earth’s surface and radiation within the human body.
MANMADE (ARTIFICIAL) RADIATION • Ionizing Radiation created by humans for various uses is classified as manmade, or artificial, radiation. • Sources of artificial ionizing radiation include: • Consumer products containing radioactive material (ie. airport surveillance systems) • Air Travel (brings humans in closer contact to extraterrestrial radiation and sunspot activity) • Nuclear fuel for generation of power (does not contribute much to annual equivalent dose of the U.S. Population) • Atmospheric fallout from nuclear weapons (also has a negligible impact on the U.S. population • Nuclear power plant accidents (ie. Three Mile Island and Chernobyl) • Medical Radiation (ie. Diagnostic medical x-ray and nuclear medicine procedures) • Manmade radiation contributes about 65mrem to the average annual radiation exposure of the U.S. population.
Basis of Effective Dose Limiting System The concept of radiation exposure and associated risk of radiation-induced malignancy, is the basis of the effective dose limiting system.
Radiation Protection Standards Future radiation protection standards are expected to continue to be based on risk.
Radiation Protection Guidelines Because medical imaging professionals share the responsibility for patient safety from radiation exposure in the performance of their duties, they must be familiar with previous, existing and new guidelines.
Major Organizations Involved in Regulating Radiation Exposure • The UNSCEAR and the NAS/NRC-BEIR supply information to the ICRP. • The International Commission on Radiological Protection (ICRP) makes recommendations on occupational and public dose limits.
National Council on Radiation Protection and Measurements • The NCRP reviews ICRPrecommendations and implements them into U.S. radiation protection policy.
The Nuclear Regulatory Commission • The NRCis thewatchdog of the nuclear energy industry; it controls the manufacture and use of radioactive substances.
Environmental Protection Agency • The EPA develops and enforces regulations pertaining to the control of environmental radiation.
Food and Drug Administration • The FDA regulates the design and manufacture of products used in the radiation industry.
Occupational Safety and Health Administration • The U.S. Occupational Safety and Health Administration (OSHA) functions as a monitoring agency in places of employment, predominantly in industry. • OSHA regulates occupational exposure to radiation through Title 29 of Part 10 of the U.S. Code of Federal Regulations (29 CFR 1910).
Radiation Safety Committee and Radiation Safety Officer • Radiation Safety Committee (RSC) • They established the facility to assist in the development of radiation safety program • The radiation safety program ensure adequate safety of patient and radiation workers.
Radiation Safety Officer (RSO) • Normally a medical physicist, radiologist, or other individual qualified training and experience. • The RSO is responsible for developing a radiation safety program for the facility to ensure that all persons are protected from radiation.
The Effective Dose Limiting System (EfD) • EfD limiting system is the current method for assessing radiation exposure and associated risk of biologic damage to radiation workers and the general public. • EfD concerns the upper boundary dose of ionizing radiation that results in a risk of body injury or genetic damage. • Expressed of whole body exposure, partial body exposure, and exposure of individual organs.
The RSO is also is responsible for maintaining radiation monitoring records for all personnel • Providing counseling for individuals who receive monitor reading in excess of allowable limits. • The RSO also have to authority to stop exam that he or she considers unsafe to personnel or patient.
The effective dose limits are established to minimize the risk to human in terms of non-stochastic and stochastic effects.
Non-Stochastic Effects • Are biologic somatic effects of ionizing radiation that can be directly related to the dose received. • The effect exhibits a threshold dose below which the effects does not normally occur • Which the biologic damage increases as the dose increases.
Early Non-Stochastic Few hours or days after a very high level radiation exposure to the body Redness on the skin (erythema) Decrease in white blood cell count. Loss of hair (epilation) Late Non-Stochastic Occurs in months or years after high level radiation exposure . Cataracts Organ atrophy Reduced fertility Sterility caused by a decease in reproductive cells Early and Late Non-Stochastic Effects
The ALARA Concept • In 1954 the National Committee on Radiation Protection put the principle that radiation exposure should be kept “As Low As Reasonably Achievable” ALARA • The medical radiographers and radiologist share the responsibility to keep occupational and non-occupational dose limits as low as possible.
The ALARA concepts presents an extremely conservative model with the respect to relationship between ionizing radiation and potential risk.
Radiation Protection • Prevention any nonstochastic (deterministic) effects by keeping dose limits below threshold levels • Limiting risk of stochastic response to conservative levels according to environment importance
Risk • Risk- probability of injury, ailment, or death resulting from an activity • Risk in medical imaging industry is possibility of inducing a radiogenic cancer or genetic defect after irradiation • Occupational risk associated with radiation exposure may be equated with risk in other industries that are generally considered reasonably safe • Risk of embryo-fetus to radiation exposure due to there high sensitivity to radiation can cause major defects
Effective Dose Limiting System • EfD is an attempt to equate the various risk of cancer and genetic effects to tissues or organs that are exposed to radiation • Equivalent dose- determination dose for all radiation-vulnerable human organs that contribute to potential risk • Tissue weighting factor indicates the ratio of risk of stochastic effects attributable to irradiation of given organ or tissue to total risk when the whole body is uniformly irradiated
NCRP Recommendations • Annual occupational effective dose limits should not exceed 50mSv (5 rem) for whole body dose • Cumulative effective dose limits refers to lifetime effective dose age in years multiplied by 10mSv for whole body dose • Collective effective dose in description with population or group exposure using an averaging the effective dose
NCRP Recommendations (cont) • Limits of nonoccupationally exposed individuals are set at 1mSv annually for medical exposure and 5mSv for natural exposure • Limits for pregnant female radiation workers are 0.5mSv per month and entire pregnancy dose limit of 5mSv • Limits for education and training purpose for individuals under 18years of age is 1mSv annually • Negligible individual dose is 0.01mSv • Limits for tissue and organs are set differently depending on sensitivity of the organ or tissue. • Lens of the eye 150mSv(15rem) • Localized skin 500mSv(50rem)
Occupational Dose Limits • Action limits are set by health care facilities to ensure radiographers do not reach a dose limit that can be harmful • Effective dose limits for radiation workers are 50mSv (5 rem) annually • Special limits are set for highly sensitive areas of the body such as the lens of the eye and localized areas of the skin, hands, and feet to prevent nonstochastic effects
Questions • T or F/ Radiation exposure should be kept as low as possible. • True • It is important for the referring physician to carry the responsibilities for determining the medical necessity for the patient. • True
QUESTIONS • True or False. EfD enables the calculation of EqD. False (EqD enables the calculation of EfD) • The quantityof _______________ radiation present in any area depends on the composition of the soil or rocks in that geographic area. TERRESTRIAL