Dive Travel
610 likes | 884 Views
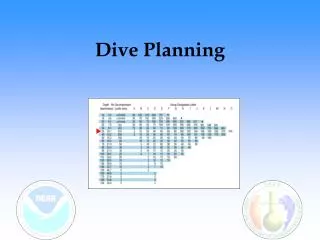
Dive Travel. Edmond Kay MD. Acknowledgements. Dr Richard Moon, Divers Alert Network Jack Connick, Optical Ocean. Declarations. Topics. Before traveling fitness issues medication While traveling DAN dive & travel insurance region specific precautions Unwanted souvenirs nasties

Dive Travel
E N D
Presentation Transcript
Dive Travel Edmond Kay MD
Acknowledgements • Dr Richard Moon, Divers Alert Network • Jack Connick, Optical Ocean
Topics • Before traveling • fitness issues • medication • While traveling • DAN dive & travel insurance • region specific precautions • Unwanted souvenirs • nasties • Bubble trouble • decompression illness
Boyles Law Pressure and Volume - Inversely Proportional
Henry’s Law Amount of gas dissolved in a liquiddirectly proportional to the partial pressureof that gas On surface On decent At pressure
Recreational Diving: DCS and Death N Divers Alert Network, 1998
What kind of Diving “Fitness to dive should apply only to the type of diving in which the diver plans to engage” - David Elliott, MD, OBE Moon RE
What kind of Diver • Not fit right now- dehydration, fatigue, URI, pregnancy • Not fit withoutspecial training • ADA - accommodation - supervision Adapted from Moon RE
Fitness to Dive • Able to do the “work”: breathe, swim, exercise • Not susceptible to barotrauma:ear, lung, GI • Not susceptible to loss of consciousness (drowning): convulsions, insulin dependent diabetes, heart block • Not pregnant • No diseases that diving could make worse:sinus or middle ear disease, previous labyrinthine window rupture, heart failure • Not ‘overly’ susceptible to DCI Age? Female gender? Obesity? Menses? Previous decompression illness? Fatigue, dehydration? Orthopedic injuries or surgery? Atrial septal defects, PFO? Moon RE
Psychological & Behavioral Fitness? • Able to exercise good judgment • Not susceptible to disabling anxiety • No sedating drugs - alcohol & tranquilizers • ADHD - oppositional & defiant • Psychosis, Mania
How to Determine Fitness to Dive “If you don’t have gills, the term ‘fitness to dive’ is a misnomer”- Andy Veale MD • What incremental risk is acceptable? • Where should the threshold for qualification be set? "It's probably more important to ask if someone has ever run out of gas on the freeway than to ask about most medical conditions” - Tom Neuman MD Adapted from Moon RE
Squeeze • MIDDLE EAR SQUEEZE • MIDDLE EAR OVERPRESSURE (REVERSE BLOCK) • EXTERNAL EAR SQUEEZE • SINUS SQUEEZE • SINUS OVER PRESSURE (REVERSE BLOCK) • TOOTH SQUEEZE (BARODONTALGIA) • BODY (SUIT) / FACE (MASK) SQUEEZE • STOMACH / INTESTINE • INNER EAR BAROTRAUMAS • PULMONARY OVER INFLATION SYNDROMES
Ear Barotrauma • Most frequent diving injury • Common in novice divers • Poor understanding of equalization techniques • Middle Ear Barotrauma is… Preventable
What is “Ear Fear”? • Pressure perceived as “uncomfortable” • Childhood pain adult fear • Retrograde tear duct inflation • Confusion over instructions
Assessing Valsalva Effectiveness • Watch The Nose Inflate! • Fingers low on nose • Palpate firmness of inflationand compare it to your own pressurization effort • Watch the pars flaccidaof the Tympanic Membrane balloon out,“like a sail catching the wind”
Video Otoscopy divingdoc.com
Ear Clearing Techniques • Valsalva Maneuver (1704) • Frenzel Maneuver (1932) • throat piston • BTV (Voluntary Tubal Opening) • distilled yawn • Lowry Technique (combinations) • pressurize and swallow • pressurize and yawn
Pulmonary Issues • Air Flow • Air Trapping
Maximum Voluntary Ventilationvs.Gas Density 100 75 MVV (fraction of 1 ATA) 50 25 0 0 100 150 200 50 Depth (fsw) Adapted from Moon RE
Chest CT after PBT in Divers AGE Pneumomediastinum Reuter et al. Br J Radiol 70:440, 1997
Unrestricted Clearance ? • Normal exercise tolerance • Normal PFT • Forced vital capacity (FVC) • Forced expiratory volume in 1 second (FEV)1 • No significant reversible obstruction • Improvement < 12% (BD) • Change not greater than 200 cc (BD) Moon RE
Recommendations for Diving with Asthma • No symptoms attributable to asthma • Normal physical exam • Normal spirometry before and after exercise provocative test with or without medication Elliott (Ed). Are Asthmatics Fit to Dive? UHMS, 1996
Seizure Risk • Seizures underwater are likely to be fatal • It is possible that the physiological conditions during diving (hyperoxia, hypercapnia, immersion) could lower the seizure threshold • People with recurrent seizures should not dive Moon RE
Seizure • 50% of adults with new onset seizures, normal neurological exam and brain imaging will have another seizure • Risk increased with family history, abnormal EEG, previous head injury • 14 years after a first seizure the risk of a second one is several fold greater than in the general population
Cause of Death Denoble PJ, Caruso J, Dear G de L, Pieper CF, Vann RD, 2007
Heart Failure • Immersion causes a displacement of 500-800 ml of blood from the legs into the thorax. This is even greater during cold water immersion • If the patient’s ventricle is unlikely to tolerate a sudden 500 – 800 ml transfusion, diving (swimming?) should be restricted Moon RE
Coronary Artery Disease • Patients with coronary artery disease are at risk of myocardial infarction and sudden death (60%) • Cardiac work is related to contractility, heart rate, afterload and preload. Preload is higher during immersion than in the dry • No diving if CAD. If patient has risk factors for CAD, rule out with exercise test (13 METS) Moon RE
Effect of Head and Torso Water Temperature on Hemodynamics Wester TE, et al. J Appl Physiol 106: 691, 2009
Fitness to Dive: Obesity- 2004 Diving Report NIH Definitions Based on BMI Moon RE
Irukandji Syndrome • One of the most venomous jellyfish • Severe headache, backache, muscle pains, chest and abdominal pain, nausea and vomiting, sweating, hypertension • EXTREMELY painful"rip your skin off"
Bubble Trouble Decompression Sickness Arterial Gas Embolism