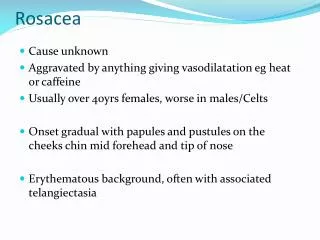
Download
1 / 102
1.03k likes | 1.05k Views
Discover the link between rosacea, gut health, and dysbiosis, exploring shared pathophysiology and treatment options. Learn about the impact of dysbiosis on the immune system and various diseases associated with bacterial overgrowth.

E N D
Rosacea and GI disordersInflammation and Dysbiosis Leonard Weinstock, MDAssociate Professor of Clinical MedicineWashington University in St. LouisSpecialists in Gastroenterology
Disclosures Speaker’s Bureau: Salix (Relistor), Ironwood (Linzess) Research grants: Salix (Xifaxan - rifaximin) Consultant: Salix (Relistor) Off label use of medicine: In context of published research and FDA IND applications for new research
“Post-infectious Rosacea” “Rosacea-SIBO” • 49 y.o. man • 3 yrHx rosacea: • E/F/Pap • Failed 2 topical Abx • Started 4 months after food poisoning • Mild bloating • Dx: bacterial overgrowth
42 F s/p Mont. revenge 13 yrs ago followed by: • E/F/Phyma and ocular rosacea • Nail disorder • IBS-c • Cognitive dysfx • Fatigue • RLS • Steatohepatitis • Type 2 DM Dx: Bacterial overgrowth
Gut microbiome • History of rosacea & gut • Small intestinal bacterial overgrowth • Enteric infections lead to diseases • Antibiotic Rx for Rosacea-SIBO • Additional SIBO diseases and rosacea • Theories for shared pathophysiology Review
Gut vs. skin • 100 SF • Barrier with vascular & nerve interface • Bacteria (100 trillion) • > 500 types • Commensal when in balance and with normal innate and systemic immunity • 10 SF • Barrier with vascular & nerve interface • Bacteria (and mites) • > 200 types • Non-invasive when in balance and with normal innate and systemic immunity
Gut + microbiome > skin + spleen Largest immune system
Normal host prevents dysbiosis Stomach 0 - 1000 oral bacteria (streptococcus, lactobacillus) Colon bacterial balance, integrity & immunity Mucosal absorption Pancreas Acid Colon 100,000,000,000,000 coliforms (bacteroides, firmicutes, bifidobacter, clostridium) Duodenum & Jejunum 1,000 oral bacteria Motility Immunity ICV Proximal ileum 10,000 oral bacteria Distal ileum 100,000,000 -1,000,000,000 coliforms Mondot. Dig Dis 2013;31:278-85.
Effects of dysbiosis • Abnormal anatomy • Leaky tight-junctions --- incr. intestinal permeability • Thinner lamina propria, shallow crypts • Abnormal Peyer’s patches, fewer plasma cells • Immune disorders: • Altered cytokine profile • Altered innate immune response (Th2 to Th1, IL-17) • Diseases: atopy, diabetes, obesity, autoimmune
Bateman. Color Atlas of Dermatology. 1817. Text: “Rosacea and acne. Constipation.”
History of rosacea and the gut • Alcohol & obesity – 13th century (Chaucer) (? Steatohepatitis) • Dyspepsia – 1895 • Food intolerance/allergies – 1926-1966 • Achlorhydria – 1935, 1941 • Gastritis – 1941 • Celiac/jejunal diseases – 1965, 1970 • Chronic pancreatitis – 1982 • H. pylori – 1990’s • IBD: UC 1989; CD 2000 (drug-induced, PPR, R. fulminans, granulomatous R.) • Small intestinal bacterial overgrowth: 2008
Early text and rosacea- associated disorders Kaposi. Pathology and Treatment of Disease of the Skin. 1895.
Textbooks and rosacea- associated disorders • GI disorders (dyspepsia, diarrhea, constip) 1 • H. pylori: • Coincidental 2, 3, plausible 4, undecided 5 • Parkinson’s disease 1, 2 • Hormonal changes 3 • Menopause 2 • Migraine 1-3 • Orthostatic hypotension 1 • Vasoactive tumors 2 • HIV 4, 5 • CNS tumors 1 Pelle. In Fitzpatrick 2012. Webster. InBolognia 2008. InMcKae 2005. Berth-Jones. In Rooks 2004. Plewig, Klingman. In Acne and Rosacea 2000.
Small intestinal bacterial overgrowth and rosaceaFirst report in 2008
SIBO syndrome • Definition • >105 colony forming units/mLin jejunum • Sx and/or signs of malabsorption • Treat 1o small bowel abnormality • “Often impractical” • Antibiotics • Absorption and resistance concerns • Motility drugs • Limited medications • Intestinal permeability • Not addressed Gregg CR, Toakes PP. InSleisenger and Fortran. Gastrointestinal and Liver Disease.
Lactulose breath test Early rise in H2 (or CH4) in SIBO gas chromatography • No gold standard to Dx SIBO - culture problems • Bacteria may be in various locations in the small bowel • Difficult to culture anaerobes
SIBO – full blown • Symptoms • Pain • Bloating • Diarrhea • Foul flatus • Weakness • Weight loss • Signs and Labs • Edema • Anemia • Cachexia • Iron def. • Vitamin def. • Nutrient def.
“New” SIBO • Crohn’s dis. * • Celiac dis. * • Irritable bowel synd. * • Chronic liver dis. * • Restless legs synd. • Rosacea • Parkinson’s dis. * • *Associated with rosacea • Renal failure • Hypothyroidism • Acromegaly • Post-chemotherapy • Fibromyalgia • Rheumatoid arthritis * • Interstitial cystitis • Chronic prostatitis Weinstock. Dig Dis Sci 2010;55:1667-73.; Weinstock. Inflam Bowel Dis 2010;16:275-9.; Pimentel. N Engl J Med 2011;364:22-32. Walters, Weinstock. Sleep Med 2011;12:610-3.; Bellot . Liver Int 2013;33:31-9.; Parodi. ClinGastroenterolHepatol 2008;6:759-764.; Fasano. MovDisord 2013;28:1241-9.; Weinstock. Dig Dis Sci2008;53:1246-51.; Geng. Can J Urology 2011;18:5826-30.
Diseases after GI infections • Guillain-Barré syndrome • Celiac disease • Reactive arthritis • Pancreatitis • IBS – 20% recall infection first Molecular mimicry & autoimmune pathways with genetic predisposition • Koga. J Infect Dis 2006;193:547-55. • Yu. Rheum Dis ClinNoth Am 2003;29:21-36 • Stene. Am J Gastroenterol 2006;101:2333-40.
Post-infectious IBS & associated syndromes Genetic phenotype (low IL-10) for IBS
Pi-IBS • 7 studies/2056 people: incidence 7-30% • Duration: 50-100% life-long (2 studies) • Pathophysiology: • Weak MMC leads to SIBO • Rat model: Camphylobacter caused SIBO in 27% • Anti-vinculin antibody studies • Rats AVA led to loss of myenteric nerves • Patients with Pi-IBS have AVA Pimentel 2004, 2011, 2013
Anti-vinculinAb (AVA) • Vinculin - involved in adhesion between cells • Skeletal muscle and nerves • Epineurial blood vessel smooth muscle • Endoneurium endothelial cells (EC) • Theoretical role in vascular changes of rosacea and neurologic balance in neurogenic rosacea: AVA might damage EC & nerves especially in Pi-Rosacea Pimentel. Abstract. ACG; Am J Gastroenterol; October 2013. Massa et al. Muscle Nerve 1995;18:1277–84.
Inflammation in SIBO & IBS • Interleukins – IL 1ß, 6, 8**, 12 • TNF-α (inflm. & incr. intestinal perm.) • LPS (inflm. & incr. endothelial cell perm.) • T- and B-lymphocytes – imbalance/activity • Mast cells infiltration in gut • Increased histamine, tryptase and seratonin • Substance P (neuropeptide) • Integrin Beta-7 T-lymphocytes (incr. vascular perm.) • A-V Ab Riordin. Scand J Gastroenterol 1996;31:977-84. Lin. JAMA 2004;292:852-8. Hughes et al. Am J Gastroenterol 2013;108:1066-74. Martinez et al. Gut 2013;62:1160-8.
Systemic cytokines in rosacea • 60 rosacea pts vs. 25 controls • IL-18: 163 vs. 16 pg/ml (P<0.01) • IL-6 lower in rosacea • TNF-alpha numerically higher • IL-8 not measured Salamon. PrzegiLek 2008;65:371-4.
Changing roles of antibiotic Rx • 1950’s: Tetracycline • 2000: low dose doxycycline • Inhibition of matrix metalloproteinases • Inflammatory cytokine regulation • Inhibition of leukocyte chemotaxis & activation and anti-oxidation • Antibiotic effect on stratum corneumtryptic enzymes (SCTEs) • 2008: rifaximin for rosacea-SIBO Parodi et al. Am J Gastroenterol 2008;6:759-764.
Rifaximin – semi-sythetic CH3 CH3 CH3 CH3COO 22 OH OH CH3 CH3 CH3 CH3 OH OH H N CH3COO CH3O CH3 22 CH3 OH OH O CH3 O OH OH N H N CH3O N O CH3 CH3 O CH3 CH3 CH3 O Rifamycin Rifaximin O O O Rifamycin (Rifampin): Tb, Leprosy, streptococci, enterococci, staphylococci, Neisseria spp. and Enterobacteriaceae FDA-approved uses of Rifaximin: Traveler’s diarrhea and hepatic encephalopathy Target 1&2 study for IBS published in NEJM Target 3 study fully enrolled 11/15/13 EMEA – includes SIBO Pimentel et al. NEJM 2011;364:22-32. Scarpignato. Digestion 2006;73(S1):13-27.
Antibiotic Rx for SIBO • 1356 articles reviewed, 10 met incl. criteria • Rifaximin most commonly studied (8 studies) • LBT normalization rate of 49.5% (Efficacy varied by antibiotic dose) • Clinical response in 6 studies correlated with LBT normalization (SIBO eradication) Shah. Aliment PharmacolTher 2013;38:925-34.
1 week course for H2+ LBT Di Stefano. Aliment PharmacolTher2000;15:1001-8.
Rifaximin properties: benefits • Non-systemic (<0.4%) (97% fecal excretion) • Gram-pos & neg; aerobes & anaerobes • Bile > water soluble – kills more bacteria in the small intestine than colon • Kills C. difficile Huang DB, DuPont HJ. J Infection 2005;50:97-106.
Rifaximin resistance profile • Resistance • Not plasmid-mediated • Mutant resistant gut bacteria exhibit reduced viability • No clinically relevant resistance • 3 IBS-SIBO retreatment studies • Re-Rx in 2 – 7 courses: successful (83-100%; 1 - 5 year follow up) • Pimentel et al. Dig Dis Sci 2011;56:2067-72. • Weinstock. Dig Dis Sci 2011;56:3389-90. • Yang. Dig Dis Sci 2008.
SIBO in rosacea: LBT+ prevalence • Genoa, Italy: 46% of 113 consecutive rosacea clinic pts • St. Louis, MO: 51% of 63 consecutive GI clinic pts with rosacea • St. Louis, MO: 66% of 176 consecutive GI clinic pts with rosacea (incl. CH4+ pts) • Parodi et al. Am J Gastroenterol 2008;6:759-764. • Weinstock, Steinhoff. J Am Acad Dermatol 2013;68:875-6. • Weinstock. EMR review of records 2008-2013.
False positive LBT: Controls • Genoa, Italy: 3/60 age matched controls • St. Louis, MO: 3/30 healthy controls • (Lactulose gets to colon faster causes FP) • Parodi et al. Am J Gastroenterol 2008;6:759-764. • Weinstock, Steinhoff. J Am Acad Dermatol 2013;68:875-6.
Rifaximin for rosacea: 1st study • N=113 pts seen in Rosacea Clinic • 83 F, 31 M, age 52 • 52/113 (46%) LBT+ • 24/113 H.p.+ (7 had SIBO) • 7 pts treated for H.p. 1 mo after SIBO Rx (clinical response occurred with SIBO Rx) • GI sx response analyzed Parodi et al. Am J Gastroenterol 2008;6:759-764.
Rifaximin for rosacea • N = 52 LBT+ (H2 excretion) • Rifaximin 1200 mg/d/10d vs. Placebo • Randomized, blinded only to pts • IGA scoring • 2 dermatologists (Kappa = 0.97) • Additional studies • Cross-over for placebo group • Open label used for SIBO-negative pts • Subtype rosacea evaluated Parodi et al. Am J Gastroenterol 2008;6:759-764.
Randomized study results • Rifaximin normalized LBT in 28/32 • 71% cleared rosacea (GA score 0) • 21% marked impr. (GA score 1) • Placebo 2/20 worsened, rest unchg. • GI sx sig. decreased with rifaximin Parodi et al. Am J Gastroenterol 2008;6:759-764.
Before & 1 mo after 1200 mg/d/10d rifaximin Courtesy of V. Savarino: Paroldi et al. Clin Gastroenterol Hepatol2008;6;759-6.
Before & 1 mo after 1200 mg/d/10d rifaximin Note periocular and cheek improvement Courtesy of V. Savarino: Paroldi et al. Clin Gastroenterol Hepatol2008;6;759-64.
Additional study results • X-over: placebo group treated open-label • 17/20 LBT normalized • 15 of the 17 had rosacea cleared • 45/52 total eradication with rifaximin • 35/45 cleared • Improvement maintained in 96% at 9 mo • 2 w pap/pustreturned & Re-Rx worked • LBT- group treated (see next) Parodi et al. Am J Gastroenterol 2008;6:759-764.
(N=32) (N=20) Rifaximin 1200 mg/d/10d Parodi et al. Am J Gastroenterol 2008;6:759-764.
Rifaximin for subtypes Pap/Pust groups had SIBO > non P/P (p<0.001) Parodi et al. Am J Gastroenterol 2008;6:759-764.
Parodi study: critisms • Baseline mean IGA not stated – delta not shown • All sub-types included • Pust. +/- pap. was most impt to include (84/113 had one or both) • Study not blinded to physicians • 2 independent scores performed with high Kappa • LBT used for SIBO Dx • Potential for more false+ • Less invasive than jejunal aspiration
Second rifaximin study: methane • 15 H2+ & 15 CH4+ rosacea pts • Rx #1: rifaximin • H2 pts - most responded • CH4 pts - little or no improvement • Rx #2: metronidazole • CH4 pts - majority with complete or significant clearance • (Note: need for dual therapy in IBS-methane pts) • Parodi. UEGS. Abstract 2008.
Rifaximin for rosacea: St. Louis • N=63 pts (59 from screening colonoscopy) • Dx by dermatolgist in 57; ETR in 50, PP in 9, refractory ocular in 4 (3 had E) • Most did not have GI sx • 32/63 pts (51%) had LBT+ vs. 3/30 controls (RR, 5.0; 95% CI, 1.7-15.1; P<0.001) • 28 LBT+ pts given rifaximin 1200 mg/d/10d • Limitations: open-label, self-assessment by questionnaire and photos by pts • Weinstock, Steinhoff. J Am Acad Dermatol 2013;68:875-6.
Improvement: self-assessed 46% 25% 18% 11% Cleared Moderate Mild Unchanged or Marked • Weinstock, Steinhoff. J Am Acad Dermatol 2013;68:875-6.
Before & 1 mo after rifaximin 1200 mg/d/10d Significant change in nose & pruritic rash over right eyebrow – patient seen 1 year later & both areas were clear
Ocular rosacea Post-infectious ocular rosacea: 1 mo after rifaximin 1200/mg/day/10d
Subsequent patient experience • Higher dose to match IBS studies and additional Rx for complex pts: • Rifaximin 550 mg TID for 14 days • Comprehensive post-SIBO Rx for complex patients
Before & 5 wk after rifaximin 1650/mg/d/14d Case 2 Eyes, RLS fatigue, memory, and nail strength Improved.