Download
1 / 34
370 likes | 925 Views
Dislocation after Total Hip Replacement Etiology and management. Pekka Ylinen ORTON/ Invalid Foundation. Dislocation. leaves a patient apprehensive tarnishes a surgeons reputation cause extra cost to health care system. Dislocation. incidence

E N D
Dislocation after Total Hip Replacement Etiology and management Pekka Ylinen ORTON/ Invalid Foundation
Dislocation • leaves a patient apprehensive • tarnishes a surgeons reputation • cause extra cost to health care system
Dislocation • incidence • risk factors (patient, surgical, implant) • diagnosis • principles of treatment • case presentations
Dislocation after THR • overall incidence 2-3% (0,4-11%) • in elderly (even 4% if older than 80 y) • females ( f:m ~ 2:1) • in revision 10-20%
Dislocation after THR Patient factors • age • female gender • prior surgery • DDH, prior fracture • neuromuscular disorders • dementia • low grade infection • alcohol abuse
Dislocation after THR Surgical factors • component malpositioning • offset not restored • failure to preserve abductor mechanism • leg length not restored • posterior approach
Risk factors suspected: • bilaterality • weight • leg length difference
Dislocation after THR Implant factors • neck design - neck cross section - offset - Morse taper length • small head • skirted head • std. acetabular design vs. elevated cup wall skirt poor head-neck ratio
Dislocation after THR • greatest risk within the first few weeks after op. - 60%-80% occur in three months - component malorientation • late instability - 23% after one year, 14 % after 5 years - loss of soft tissue integrity
Dislocation rate vs. head size and surgical approach Woo, Morrey JBJS (Am) 64:1295, 1982
Dislocation after THR Rates according to surgeon volume • 1-5/year 4,2 % • 6-10/year 3,4 % • 11-25/year 2,6 % • 26-50/year 2,4 % • > 50/year 1,5 % JBJS (Am) 83:1622, 2001
Surgical approach and THR dislocation • controversial according to literature - quality of orthopaedic literature recarding THR dislocation is limited - no prospective studiesof sufficient power exist • 14 articles fulfilling 5 to 8 inclusion criteria: - 3,23% for the posterior approach - 0,55% for the direct lateral approach Clin Orthop 405, 2002
Treatment • modular component exchange • trochanteric advancement • bipolar rearthroplasty • jumbo femoral heads • constrained acetabular components
Modular component exchange For patients who do not have malpositioning of the components or abductor dysfunction • increasing neck lenth • increasing femoral head size • using more lipped and/or reoriented liners be aware about - malposition - impingement ?
Effectiveness of Modular component exchange* * without implant malpositioning
Trochanteric advancement • in monobloc implants without option to increase neck length • proximal migration of fractured or ununited trochanter
Bipolar rearthoplasty • good in gaining stability (~ 80%) • bad in functional outcome due to articulation with exposed acetabular bone JBJS (Am) 82:1132,2001
Jumbo femoral heads • maximal head to neck ratio minimizes implant impingement • 32 mm - acetabular component size - thickness of the polyethylene • 36-38 mm ? • tripolar arthroplasty
Constrained acetabular components • restricted range of motion and impingement • thin polyethylene • outcome maybe implant dependent? - Osteonics: loosening 2% dislocations 4% J JBJS (Am) 80:502, 1998 - S-Rom: loosening 4% dislocations 9-29% J Arthroplasty 9:17,325, 1994
Treatment strategy Unstable THR Implant malposition Implant in good position Impingement Abductor dysfunction Revise laxity non-union incompetent Modular exhange Lipped poly Anterverted poly Lateralized poly Longer neck Trochanteric advancement Refixation Constrained cup Large head
First dislocation: treatment strategy • identify the direction of instability • determine the cup orientation with C-arc • cup orientation acceptable, one-half hip brace for 6 to 8 weeks • anterior dislocation: cup in 20° - 30° anteversion, one half hip brace for 6-8 weeks • posterior dislocation: cup in retroversion, cup revision
Cup orientation • direct ap-view: if anterior and posterior rims are coincident the orientation is about 6° in anteversion
Cup orientation 45°
Cup orientation • the position of C-arc when the anterior and posterior rims are coincident shows the cup orientation
C-arc fluoroscope X-rays (C-arc) 13° to 15° anteverted x-rays (C-arc) vertical
male, 58 years trochanteric advancement
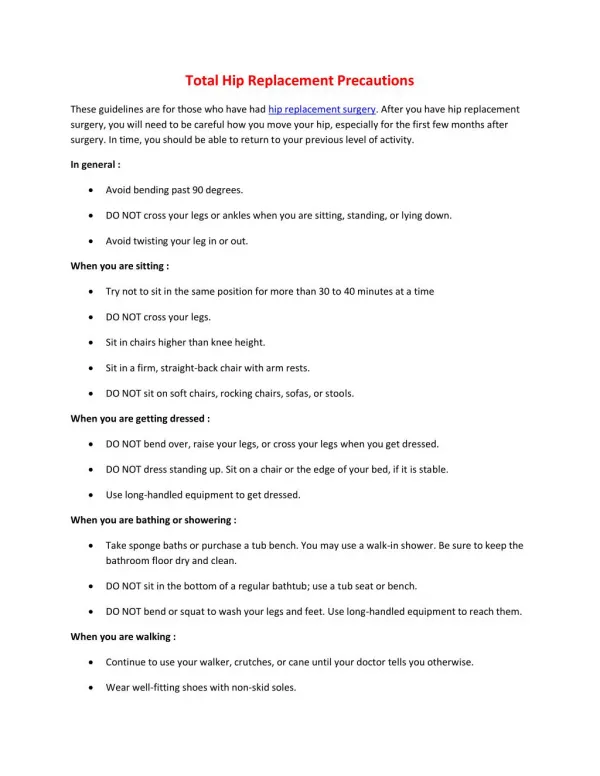
Prevention on hip dislocation • identify patient at risk • restore femoral head offset • larger femoral head • restore leg length • proper postoperative care