MANOMETRY Measurement Technique
MANOMETRY Measurement Technique. Jia-Feng Wu, M.D. Division of Gastroenterology, Department of Pediatrics, National Taiwan University Children Hospital. Manometry at NTUH. 1985. 2007. Manometry. Anorectal manometry Esophageal manometry Antroduodenal manometry Oddi sphincter manometry.


MANOMETRY Measurement Technique
E N D
Presentation Transcript
MANOMETRY Measurement Technique Jia-Feng Wu, M.D. Division of Gastroenterology, Department of Pediatrics, National Taiwan University Children Hospital
Manometry at NTUH 1985 2007
Manometry • Anorectal manometry • Esophageal manometry • Antroduodenal manometry • Oddi sphincter manometry
Anorectalmanometry • Indication • Equipment • Preparation • Investigation • Analysis
Anorectalmanometry • Indication • Fecal incontinence • Constipation • Evaluation before-after operation • Equipment • Ano-rectal motility probe • Recording device • Computer • Software
Anorectalmanometry • Equipment • Ano-rectal motility probe • 3, 4, 6 or 8 channels • Balloon • Water perfused • Micro-tip (not very common)
Catheter • Equipment • Ano-rectal motility probe • MicroTip catheter • 1-4 channels • Balloon mounting ring
Preparation • Preparation • Patient must empty bladder and rectum. Enema only needed if patient has severe constipation • Connect catheter to perfusion system • Flush all channels to remove air-bubbles • Zero balance catheter at anal sphincter level • Introduce catheter in Anal sphincter/rectum • Ready to start…...
Investigation • Investigation • Resting/Relax pressure • Squeeze pressure • Endurance squeeze • Push/strain pressures • Cough test • RAIR • Sensation test • Vector Volume/Profile
Resting • Investigation • Resting/Relax pressure • Let the patient rest, no squeeze for 30 seconds • Analyze average resting pressure in the high pressure zone (IAS and EAS)
Squeeze • Investigation • Squeeze pressure • Ask patient to squeeze for about 5 sec • Wait 30 sec and repeat 3 times • Analyze EAS contraction
Endurated squeeze • Investigation • Endurance Squeeze • Ask patient to squeeze for about 25 sec • Analyze fatigue slope of EAS
Push • Investigation • Push/Strain pressure • Ask patient to strain like to defecate • Pitfall: embarrassment of patient • Analyze EAS relaxation
cough • Investigation • Cough test • Ask patient to cough • Analyze EAS contraction in response to sudden increase of abdominal pressure
RAIR • Investigation • RAIR (Recto-Anal-Inhibitory-Reflex) • Inflate balloon (20-50 mL or stepwise 0-10-0-20-0-30-0-40-0-50 with air) • Analyze IAS relaxation and spontaneous EAS response
Sensation • Investigation • Sensation test • Inflate balloon with air stepwise +10 ml (10, 20, 30, 40...250 mL...until Max Vol) • Wait 20-30 sec between inflation for accommodation of the rectum • Ask patient sensation (No sensation, First sensation, urge, max Tolerable volume
Normal data in children J Pediatr Surg 2009;44:1786-90
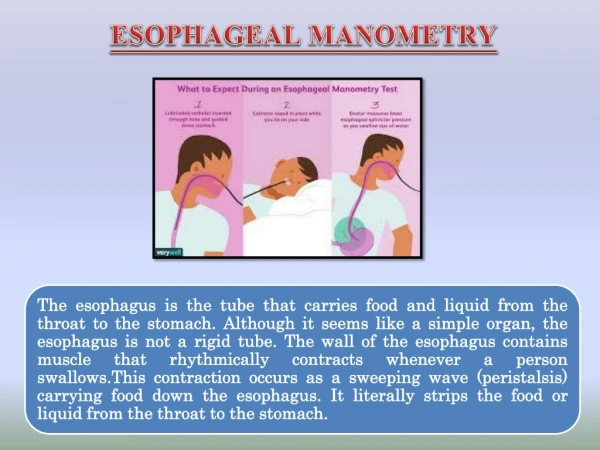
Esophageal manometry • Anatomy • Indication • Equipment • Preparation • Investigation • Analysis
Esophageal manometryindication • Primary esophageal motility disorders • Achalasia • Nutcracker esophagus • Diffuse esophageal spasm • Hypertensive LES • Nonspecific Esophageal motility disorders • Secondary esophageal motility disorders • Scleroderma • Diabetes mellitus • Chronic idiopathic intestinal pseudo-obstruction • Autoimmune disease
Esophageal manometry -indications • Determination of LES prior to pH investigation • Pre-operative to exclude motility disorders for anti-reflux operations • Dysphagia
Catheter • Equipment • Esophageal motility probe • 4-8 channels • 5 cm spacing • Sleeve at the tip
catheter • Equipment • Esophageal motility probe • MicroTip catheter • 3-6 channels
Preparation • Preparation • Patient must fast at least 6 hours • Connect catheter to perfusion system • Flush all channels to remove air-bubbles • Zero balance catheter • Lubricate catheter and introduce via the nose • Ready to start…...
investigation • Investigation • LES: • Gastric baseline pressure • LES resting pressure • LES borders (location) • LES relaxation during swallow • Esophagus: • Esophageal motility (peristaltic contraction) • UES: • Relaxation during swallow
Steps • All channels in stomach; withdraw the catheter stepwise (0.5 cm/withdraw) and mark distances • Look for the lower/upper border of the LES • Position channels in esophagus and LES • Let the patient swallow 10x (dry and wet swallow) • Mark wet and dry swallows • Optional UES
interpretation • Amplitude of primary peristalsis: 48±7 mmHg secondary peristalsis: 46±5 mmHg • Wave onset to peak (promixal): 1.9±0.1 secs (distal): 1.8±0.1 mmHg • Velocity of primary peristalsis: 1.2-2.5 cm/s secondary peristalsis:6.2-7.9 cm/s • Percentage of abnormal wave: < 15% contractions Am J Gastroenterol 2009;104:411-419
Motility disorder • Hypomotility Disorders Achalasia • Hypermotility Disorders Diffuse Esophageal Spasm • Hyperperistalsis Nutcracker • Nonspecific Esophageal Motility Disorders
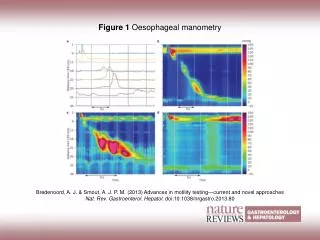
Esophageal spasm Manometry Esophagography
Esophageal spasm • Manometry findings: Peristalsis:>30% abnormal contractions Duration and amplitude occasionally abnormal LES: occasional hypertensive; occasional incomplete relaxation
Achalasia Manometry Esophageography 37
Achalasia • Esophageal manometry findings: normal or increased resting pressure Incomplete or absent relaxation decreased distal contraction amplitude increased resting esophageal body pressure
Nutcracker Esophagus Manometry Esophagography
Nutcracker Esophagus • Manometry findings: Normal peristalsis Contraction amplitude is > 2 SD above normal > 180 mmHg in distal esophagus Duration of contractions >6 sec. LES: occasional hypertensive; usually normal