Download
1 / 43
440 likes | 465 Views
Learn about Leishmania, a flagellated protozoan causing Leishmaniasis, and Giardia, a parasite causing Giardiasis. Explore their morphology, life cycle, pathogenesis, clinical features, diagnosis, treatment, prevention, and more.

E N D
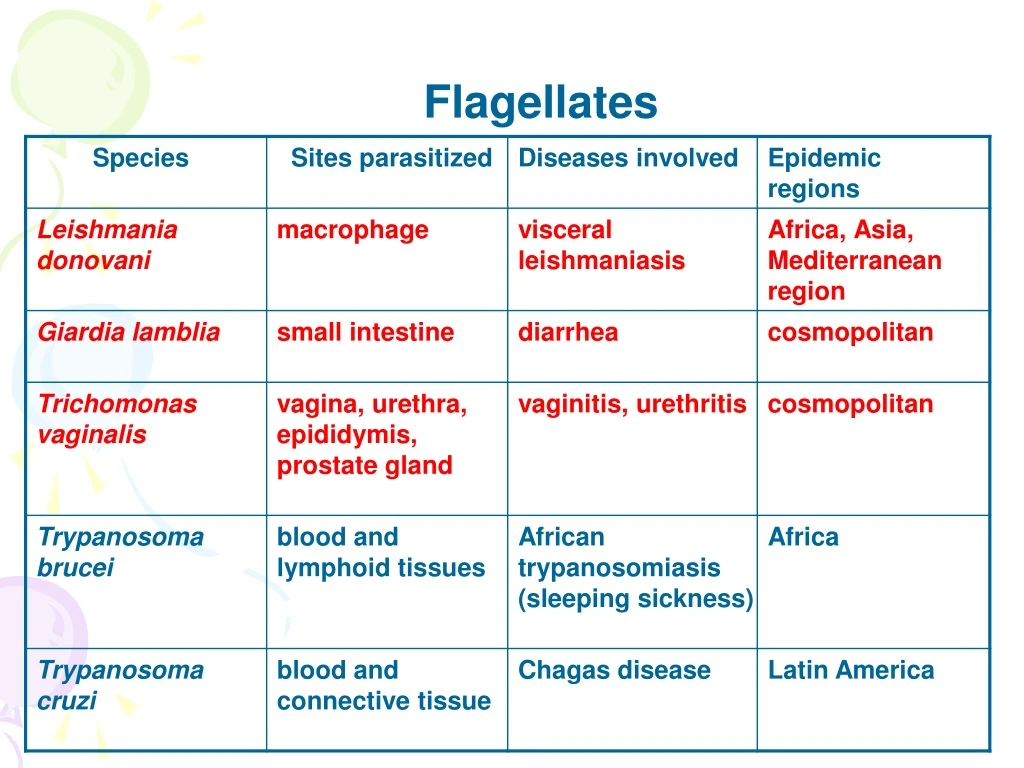
Introduction • Leishmania is a kinetoplastid flagellate • Inhabits macrophages • Leishmaniasis (Kala-azar, black fever) is a zoonosis transmitted by the bite of sandflies • Leishmaniasis affects 12 million people in 88 countries, 4 million new cases per year
Introduction • Three main forms of leishmaniasis • Visceral : involving liver, spleen, and bone marrow –Leishmania donovani • Mucocutaneous : involving mucous membranes of the mouth and nose –Leishmania braziliensis • Cutaneous : involving the skin at the site of a sandfly bite –Leishmania tropica, Leishmania mexicana, Leishmania major
MucocutaneousLeishmaniasis nasal mucosa and septum are involved Leishmania braziliensis
CutaneousLeishmaniasis • Oriental sore • Eastern Mediterranean • Self-cured disease, sterilizing immunity • Leishmania tropica, Leishmania mexicana, Leishmania major
Endemic Areas for Leishmaniasis BMJ 2003;326:378
Cutaneous Leishmaniasis Visceral Leishmaniasis
Morphology Leishmania donovani • Minute elliptical body, 2-5µm • Very short flagellum barely beyond the cell surface • Single prominent nucleus – located at one side • Cytoplasm- containing kinetoblast; basal body 1.Amastigote (Leishman-Donovan body, LD body)
Amastigote Morphology • Bone marrow smear -- Giemsa stain
Morphology Large numbers of amastigotes in a M
Morphology • M broken with the release of amastigote which may invade other M, start asexual multiplication again Amastigote
Morphology 2.Promastigote • Fusiform-shaped with 1 free flagellum • Usually gather together in the medium as a mum
Life cycle • 2-host pattern, mammal insect vector • Asexual multiplication occurred either in macrophages or in insect • Blood feeding of female sandfly, bring amastigote to vector host gut • AmastigotePromastigote(3d) binary fission to fill the mouth part (7d)
Life cycle • Macrophagesbring proliferated amastigotes all over the body • Dogs and rodents may serve as a reservoir hosts • Amastigotes may also be transferred by blood transfusion
Life cycle Phlebotomus,sandfly • Small,about 1/3 of a mosquito, 3mm, yellow-gray
Pathogenesis • Mechanism of parasites entering macrophages • Mechanism of hypersplenism Anemia, leukopenia, and thrombocytopenia
Clinical features • Infections range from asymptomatic to progressive, fully developed kala-azar. • Incubation period is usually 2 – 4 months. • Symptoms – Begin with low-grade fever and malaise, followed by progressive wasting, anemia, and protrusion of the abdomen from enlarged liver, spleen and lymph nodes. • Nephrosis: IC deposition –type III hypersensitivity
Clinical features • Fatal after 2 – 3 years if not treated. • Immediate cause of death is usually an invasion of a secondary pathogen that the body is unable to combat. • Gain acquired immunity after effectively cured • In acute cases with chills, fevers up to 40 ℃ and vomiting; death may occur within 6–12 months.
Two children with visceral leishmaniasis Splenomegaly
Special clinical features for Kala-azar cases • Post-kala-azar dermal leishmaniasis (PKDL):
Diagnosis • Etiological examination • Puncture smear: bone marrow – safe, first choice • Skin biopsy • Tissue or aspirate cultivation • Animal inoculation
Animal Xenodiagnosis hamsterinfected with L.donovani
Diagnosis • Immuno-diagnosis • Antibody detection • Circulation antigen detection • Molecular biology methods • DNA probe test • PCR
Treatment • Injection of Antimony Gluconate(葡萄糖酸锑钠)cure rate would be 97.4%。 • Pentamidine or stilbamidine for antimony-resistant patients • Spleen excision
Prevention • Treat the patients • Suppress the reservoir: dogs, rats, gerbils, other small mammals and rodents • Suppress the vector: Sandfly • Prevent sandfly bites: Personal Protective Measures • Most important at night • Sleeves down • Insect repellent • Permethrin soaked uniforms • Permethrin soaked bed nets
Introduction • Flagellated protozoan parasite • Colonizes and reproduces in the small intestine • Cause giardiasis (travelers diarrhea) • Person to person transmission • Commoninmanydevelopingcountries
Morphology Nucleus Adhensive disc Medianbody flagellum axostyles trophozoite
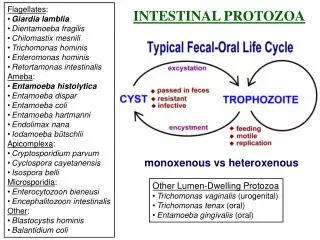
Life cycle • Trophozoites in duodenum, jejunum and upper ileum • Rapid division to produce large number • Infective stage: mature cyst • Infective route: fecal-oral transmission • Infected person may produce approximately 9 billion cysts per day, which are passed in feces • Infection occurs after oral ingestion of as few as 10 to 25 cyst
Pathogenesis • Asymptomatic cyst passer (5 to 15%) • acute self-limited diarrhea (25 to 50%) • chronic syndrome of diarrhea • malabsorption and weight loss • Symptomatic giadiasis is characterized by • acute onset of diarrhea • abdominal cramps, bloating and flatulence • feelings of malaise,nausea • vomiting, fever and tenesmus occur less commonly • stools may be profuse and watery, but later they are commonly greasy, and foul-smelling • Vitamin B12 deficiency
Diagnosis • Wet, saline mounts: trophozoite (Symptomatic giadiasis ) • Iodine dye techniques: cyst (Asymptomatic cyst passer ) • Biopsy tissue/duodenal aspirate stained by Giemsa stain • Enzyme immunoassay and fluorescent-antibody monoclonal antigen detection system
Epidemiology • Presumed to be zoonotic, but new evidence indicates that strains may be species specific • Host can be humans, primates, cat, dog, beaver, rabbits, etc. • World wide distribution • Highest incidence in children, young adults and travelers in late summer
Prevention and treatment • Treat the patients and carrier • Proper handling and treatment of water • Good personal hygiene on an individual basis • Metronidazole, Quinacrine, Furazolidone, Paromomycin and Tinidazole
Introduction • A sexually transmitted infection • Only trophozoite stage in life cycle; no cyst form • Resides in urogenital tract • Trichomoniasis: vaginitis in women, while urethritis in men • Wet, saline mounts: trophozoite • 160 million cases of infection are acquired annually worldwide (WHO, 2011) • Cured with metronidazole or tinidazole