International Neonatal Immunotherapy Study
300 likes | 451 Views
International Neonatal Immunotherapy Study. National Perinatal Epidemiology Unit Oxford www.npeu.ox.ac.uk. Co-ordinating centre. INIS is run by the National Perinatal Epidemiology Unit, Oxford Please visit our site at www.npeu.ox.ac.uk If you have any queries please contact

International Neonatal Immunotherapy Study
E N D
Presentation Transcript
International Neonatal Immunotherapy Study National Perinatal Epidemiology Unit Oxford www.npeu.ox.ac.uk
Co-ordinating centre • INIS is run by the National Perinatal Epidemiology Unit, Oxford • Please visit our site at www.npeu.ox.ac.uk • If you have any queries please contact • Barbara Farrell (Trial Director) • Clare Shakeshaft (Study Co-ordinator)
INIS – current status • Start of trial 2001 • Participating centres 97 • Participating countries 9 • Babies recruited 3,292 (March 07) • See www.npeu.ac.uk/inis for current update
INIS Co-ordinating Team Peter Brocklehurst Chief Investigator Barbara Farrell Trial Director Clare Shakeshaft Study Co-ordinator Caroline Wilson Follow up Co-ordinator Andy King Programmer Rui Zhao Data Assistant Ellie Morgan-Jones Administrative Assistant
INIS - future • Aim • To reach a target of at least 3500 babies by end of recruitment 31st May 2007
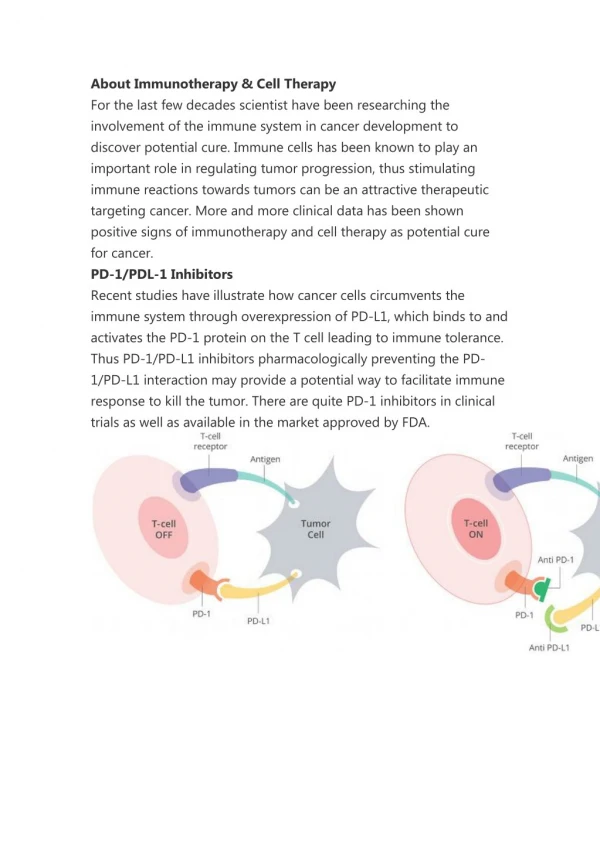
INIS hypothesis • That, in infants receiving antibiotics for clinical sepsis, the addition of non-specific immunoglobulin (IVIG) reduces mortality and major morbidity compared with antibiotics alone
INIS - study design • Gold standard for treatment trials • Double-blind • Randomised • Placebo -controlled
Receiving antibiotics and proven or suspected serious infection Placebo IVIG Mortality or major disability at 2 years
Eligibility criteria 1.Receiving antibiotics and suspected or proven serious infection AND ………
Eligibility criteria 2. At least one of the following: • birth weight less than 1500g • receiving respiratory support via an endotracheal tube • evidence of infection in blood culture, CSF or usually sterile body fluid AND………
Eligibility criteria AND ……… 3. There is substantial uncertainty that IVIG is indicated
Exclusion criteria • IVIG already given* • IVIG thought to be needed or contraindicated *specific IVIG
Specific IVIG • IVIG for specific indications should be given as per hospital policy and these infants will still be eligible • Hepatitis B immunoglobulin • Varicella-Zoster immunoglobulin
Eligibility - age • Babies at any age whilst resident on NICU • After discharge babies are eligible until EDD plus 28 days
Consent • Consent must be fully informed and obtained before randomisation • Use the Information Leaflet • Direct parents to website or INIS contact
Randomisation • Simple, no phone call required • Drug boxes in pre-randomised sequence • Use lowest numbered box
IVIG • Plasma from non-UK donors • Produced by Scottish National Blood Transfusion Service • Tested for HIV 1 ,2 and Hepatitis A,B,C • Excellent safety record • Few adverse reactions
Placebo • 0.2% albumin • Identical appearance to IVIG • Safety record as for IVIG
Follow-up • Parent questionnaire • Paediatrician questionnaire • Completed at 2 year corrected age
Primary outcomes • Death or • Major disability at 2 years corrected age
Secondary outcomes • Short term • Death, chronic lung disease or major cerebral abnormality before hospital discharge • Significant positive culture after trial entry • Pneumonia • NEC • Duration of respiratory support
Secondary outcomes • Long term • Death before 2 years • Major disability at 2yrs • Non-major disability at 2yrs
Eligible? • 29 weeks gestation • Deterioration day 34 • Recurrent apnoeic episodes • Prolonged cap. refill time • CRP 66 • Commenced on antibiotics • CNS in blood culture
Eligible? Remember • It is NOT TOO LATE to randomise an infant after a positive blood culture has been reported • IVIG may be of benefit after the inflammatory process has begun
Eligible? • 27 weeks gestation, 1.3kg • PROM 27 hrs • GBS on maternal HVS • Intrapartum antibiotics not given • Asymptomatic infant • Antibiotics commenced as hospital policy
Eligible? But • If there was offensive liquor, raised inflammatory markers or this baby was to become unwell This baby would be eligible for INIS
Eligible? • Term infant • Cyanotic episodes at 2hrs age • Apnoeic requiring ventilation • CXR patchy consolidation both lung fields • Commenced on antibiotics • CRP 19
Any Questions?Please contact us:Tel: 01865 289741 Email: inis@npeu.ox.ac.uk
References 1. Murphy DJ, Hope PL, Johnson A. Neonatal risk factors for cerebral palsy in very preterm babies: case-control study. BMJ 1997;314:404. 1. Yoon BH, Romero R, Park JS et al. Fetal exposure to an intra-amniotic inflammation and the development of cerebral palsy at the age of 3 years. Am J Obstet Gynecol 182:675-681. 2. Wu YW. Systematic Review of Chorioamnionitis and Cerebral Palsy. Mental Retard Dev Disabilities Research Reviews 2002;8: 25-29. 3. Damman O, Leviton A. Infection remote from the brain, neonatal white matter damage, and cerebral palsy in the preterm infant. Semin Pediatr Neurol 1998;5:190-201.