Download
1 / 19
190 likes | 283 Views
Research and Development in Pulmonary Fibrosis: The Future is Bright. Glenn D. Rosen, M D Associate Professor of Medicine Interim Co-Chief and Program Director Pulmonary and Critical Care Medicine Director of ILD Program. DISCLOSURES. ADVISORY Intermune Celgene

E N D
Research and Development in Pulmonary Fibrosis: The Future is Bright Glenn D. Rosen, M D Associate Professor of Medicine Interim Co-Chief and Program Director Pulmonary and Critical Care Medicine Director of ILD Program
DISCLOSURES ADVISORY Intermune Celgene Coalition for Pulmonary Fibrosis
“The test of a first-rate intelligence is the ability to hold two opposed ideas in the mind at the same time, and still retain the ability to function.” F. Scott Fitzgerald, “the Crack-Up” 1936
ATS CONSENSUS STATEMENT FOR TREATMENT OF IPF “…lack sufficient clinical evidence that any treatment improves survival or quality of life for patients with IPF” Therapy is not indicated in all patients For appropriate patients, start therapy at first clinical or physiological evidence of impairment or documentation of decline in lung function
Potential Treatments for IPF and other fibrotic lung diseases Interferon-g1b Pirfenidone Etanercept ACEIs Statins NAC Immunosuppressants Corticosteroids Antifibrotic Activity Anti-inflammatory
DESIGN OF CAPACITY TRIAL • Two concurrent, multi-national trials • Total 779 patients • CAPACITY 1 (PIPF-006) 344 patients • PFD 2403mg: Placebo (1:1) • CAPACITY 2 (PIPF-004) 435 patients • PFD 2403mg: Placebo: PFD 1197mg (2:2:1) • Primary endpoint: Change in percent predicted Forced Vital Capacity (FVC) at 72 weeks (Rank ANCOVA) • Secondary endpoints • Measures of lung function, exercise tolerance, patient-reported outcomes, etc. • Primary analysis of secondary endpoints to be pooled (2403mg vs. placebo) if primary endpoint in both studies is met • Patients continue on study until last enrolled patient completesWeek 72
PROGRESSION-FREE SURVIVAL (PFS) *Defined as Time to Death or Disease Progression (>10% decrease in FVC or >15% decrease in DLCO)
CAPACITY TRIAL: Summary In the CAPACITY 1 study, the group receiving pirfenidone had a drop in their FVC over 72 weeks of 6.49% and the placebo group had a drop of 7.23%. There was no significant difference in the change in FVC between these 2 groups. In the CAPACITY 2 study, the group receiving regular dose pirfenidone had a drop in FVC over 72 weeks of 6.49% whereas the placebo group had a drop of 9.55% which was significantly different (pirfenidone group deteriorated less). In the CAPACITY 2 study, the pirfenidone group had significantly fewer ‘events’ of disease progression (death or worsening breathing tests) than the placebo group. Next step: Await the FDA’s response to InterMune’s application for the use of Pirfenidone in patients with IPF.
Common AEs with Incidence ≥1.5 Times in the Pirfenidone vs. Placebo Groups Common AEs are defined as occurring ≥10% of pirfenidone 2403 mg patients in either study
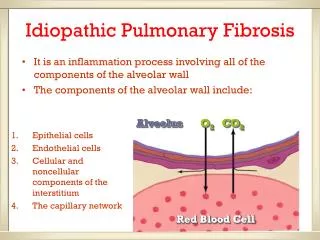
BENCH TO BEDSIDE AND BEDSIDE TO BENCH • In my laboratory at Stanford, we use samples from IPF lungs to help understand what causes IPF and to identify better treatments • Fibroblasts are isolated from lungs of patients undergoing a biopsy for diagnosis of IPF or lung transplantation and analyzed in our laboratory • We and others have discovered genes and pathways active in IPF which may help us understand why the lungs scar. Blocking these genes or pathways may lead to new treatments for IPF
SUMMARY • IPF and other fibrotic lung diseases are processes which involve lung damage and formation of excessive scar in response to this damage • Cause is unknown but likely represents a combination of genetic, environmental, aging, and unknown factors • Many clinical trials of new therapies for IPF are ongoing and planned • Pirfenidone in a Japanese and an American trial slowed disease progression, using decline in FVC as a surrogate • Keep asking questions, remain hopeful, and let Congress know that more funding is needed!
THANK YOU FOR LISTENING AND COMING TODAY! Stanford Center for Interstitial Lung Disease 300 Pasteur Drive, Rm H3143 Stanford, CA 94305-5236 Director: Glenn D. Rosen, MD Nurse Coordinator: Virginia Adi, RN Research, Database and Trials: Susan Jacobs, RN, MS and Tessa Hunter, BS Physician Colleagues: Paul Mohabir, MD and Tushar Desai, MD Phone: (650) 736-7301 or (650) 725-8082