Download
1 / 37
390 likes | 663 Views
Shingles. Jerry Hsu, Jesse Liu, Xin Yang Department of Internal Medicine Duke University Medical Center Editor: Amy Shaheen, MD Assistant Professor of Clinical Medicine Duke University Medical Center. Definitions Epidemiology Causes/Risk factors Natural history Complications

E N D
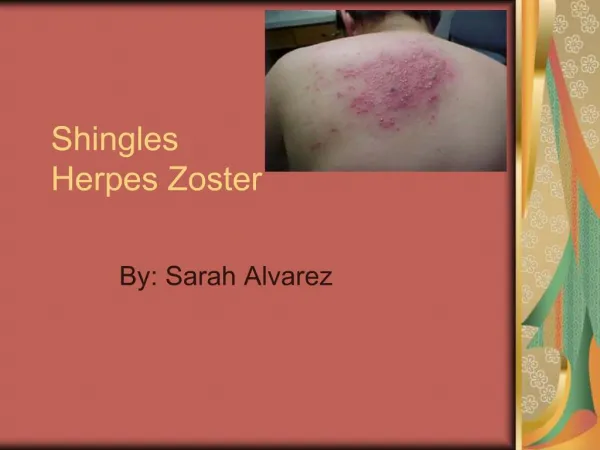
Shingles Jerry Hsu, Jesse Liu, Xin Yang Department of Internal Medicine Duke University Medical Center Editor: Amy Shaheen, MD Assistant Professor of Clinical Medicine Duke University Medical Center
Definitions • Epidemiology • Causes/Risk factors • Natural history • Complications • Screening • Diagnosis • Management • Self-Assessment Questions Introduction
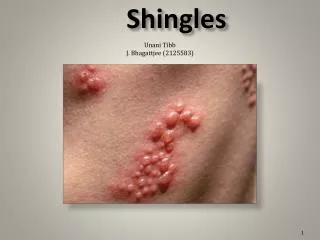
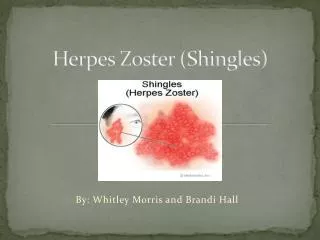
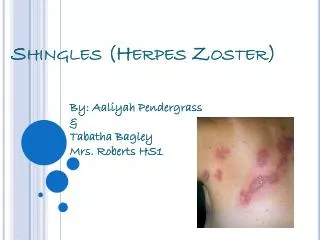
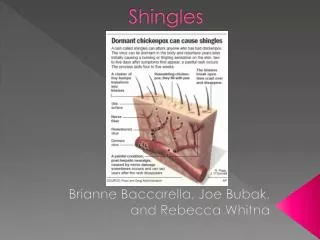
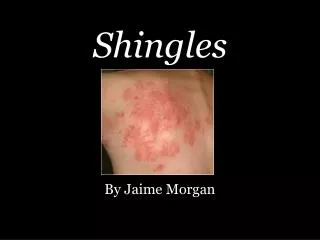
Following primary infection with varicella-zoster virus (VZV), which causes chickenpox in susceptible hosts, latent infection is established in the sensory dorsal root ganglia. Reactivation of endogenous latent VZV infection within the sensory ganglia results in herpes zoster or "shingles", a syndrome characterized by a painful, unilateral vesicular eruption in a restricted dermatomal distribution Definitions
While herpes zoster is reported in all age groups, the cumulative lifetime incidence is approximately 10 to 20 percent of the population. Overall zoster incidence rate of 215 per 100,000 person years. Both genders equally affected. In the United States, herpes zoster cases are reported in approximately 300,000 to 600,000 individuals annually, with the highest incidence (5 to 10 cases per 1,000 persons) occurring after the sixth decade. Epidemiology
Caused by reactivation of Varicella Zoster virus. • Risk factors: • Immune suppression through stress, chronic illness, HIV, malignancy • Advanced age Causes/Risk Factors
Natural History • Typically, prodrome of dysethesias, malaise, HA preceding vesicular dermatomal eruption by several days • Dermatomal rash evolves from grouped vesicles/bullae to pustular, occasionally hemorrhagic lesions within 3-4 days • Lesions crust by day 7-10 (immunocompetent hosts) and become no longer infectious • Complete resolution occurs within 3-4 wks
Ocular, neurologic, bacterial superinfection of the skin, postherpetic neuralgia • Herpes zoster ophthalmicus: a serious sight-threatening condition related to VZV reactivation in the trigeminal ganglion • Acute retinal necrosis: VZV linked as a causative organism. Features may include acute iridocyclitis, vitritis, necrotizing retinitis, occlusive retinal vasculitis with rapid loss of vision and eventual retinal detachment • Ramsey-Hunt syndrome (Herpes zoster oticus) - triad of ipsilateral facial paralysis, ear pain, and vesicles in the auditory canal and auricle • Other neurologic complications - aseptic meningitis, peripheral motor neuropathy, myelitis, encephalitis, stroke syndromes, postherpetic neuralgia Complications
Primarily based on suspicious clinical findings, usually dermatomal skin eruption, prodrome Screening
Usually based on history and physical examination • Confirmatory lab testing can be done if necessary. Cellular scrapings from the base of fresh lesions or vesicles submitted on slides to the lab are the specimen of choice for confirming diagnosis of VZV infection (The Center for Shingles and Postherpetic Neuralgia) • DFA is typically the test of choice. PCR is the most sensitive method available, but is still very expensive and not widely available. Both methods are now preferable to the old standard Tzanck smear. • VZV is hard to grow in the lab. With ideal collection, transport, and cell culture, it may require long-term incubation (up to 3 wks) to isolate the virus • Serologic methods testing for antibodies against VZV are usually not helpful in assessing recurrent VZV infection (shingles) Diagnosis
Treatment modalities • Wound care • Antiviral therapy • Steroids • Pain Control • Varicella-Zoster Vaccination Management
Wound care • Keep skin lesions clean • Sterile, nonocclusive, nonadherent dressing Management
Antiviral therapy • Acyclovir • Valacyclovir • Famciclovir • Foscarnet Management
Acyclovir • viral DNA polymerase inhibitor/nucleoside analog • use within 48-72 hours of rash onset • shown to decrease duration of acute neuritis • may decrease PHN at 6 mo • 800mg PO five times per day x 7 days Management
Valacyclovir • prodrug which is converted to acyclovir • 3-5X bioavalability vs. acyclovir • more expensive than acyclovir • TID dosing vs. 5 times per day dosing of acyclovir • in some studies, superior to acyclovir for treatment • of acute pain and decreasing length of PHN • 1000mg PO TID x 7-14 days Management
Famcyclovir • converted in GI tract to penciclovir • more expensive than acyclovir • better than placebo • equivalent to acyclovir • 500mg TID x 7 days • for ophthalmic zoster- consider valacyclovir, • famcyclovir, or IV acyclovir Management
Foscarnet • in vitro inhibitor of viral polymerase • used in acyclovir-resistant herpes zoster • 40mg/kg IV q8h x 10 days • used in immunosuppressed patients Management
Steroids • used with antivirals • does not decrease incidence/severity of PHN • accelerate healing of lesions and decrease duration • of acute neuritis • 21 day prednisone taper: 60 mg/d x 7 days, • 30 mg/d x 7d, and 15 mg/d x 7 days. • effective for patients > 50 years old and treatment • beginning within 72 hours of onset of rash • trials did not stratify by intensity of rash or pain • age group in trial chosen from demographics of shingles Management
Risks of Steroids • may weaken body’s immune system • use only in immunocompetent individuals • potential increased risk of bacterial skin infections • do not use after finishing antivirals, risk of viral • replication Management
Pain Control • NSAIDS not useful • opioids helpful: Oxycodone 5mg q6h prn, titrate up for pain • for PHN: long-acting opioids: Oxycontin 10mg q12h or • Fentanyl patch 25mcg/d which can be titrated up • Lidocaine 5% patch: apply to painful area, can use up • to 3 patches for 12 hours • Tricyclic antidepressants: nortriptyline 10mg qhs to max dose of • 150mg daily dose • Gabapentin 300mg daily, can titrate up over 4 wk period to • max dose 3600mg/d divided in 3 doses Management
Varicella-Zoster virus (VZV) vaccine • NEJM study including Durham VA headed by Ken Schmader • 1st treatment to show: • Reduced incidence of postherpetic neuralgia by 67% • Reduced the incidence of herpes zoster by 51% • Reduced burden of illness due to herpes zoster by 61% • FDA has approved vaccine for adults > 60 years old but dosage • and timing of vaccine have not been set, likely will be similar • to NEJM trial • No recommendations on vaccine by USPHTF or other groups yet • Children’s varicella vaccine dosage is too low and not been • Shown to be effective Management
Varicella-Zoster virus (VZV) vaccine • Details of study • 60 yo+ adults in randomized, double-blind, placebo controlled trial • with 0.5ml live attenuated Oka/Merck VZV vaccine given once • Pts with active herpes identified by clinical and laboratory PCR tests • Median 3 year follow up. • Primary endpoint: burden of disease • Secondary endpoint: incidence of postherpetic neuralgia • No increased side effects Management
Varicella Vaccine • Varicella vaccine is composed of the Oka strain of live, attenuated VZV • (brand name: Varivax, manufactured by Merck) • Children: 1 dose of chickenpox vaccine (0.5 mL SC) between 12-18 mo of age • or at any age if they have never had chickenpox • People who do not get the vaccine until > 13 yo, should get 2 doses (0.5 mL SC), • 4-8 wks apart • All adults who have never had chickenpox should be vaccinated • contraindications: immunosuppression, pregnancy, gelatin or neomycin allergy, • recent blood transfusions*Per CDC recommendations and American Academy of Pediatrics; not addressed by USPHTF) Management
Self-Assessment Questions 1. Which of the following is not a risk factor for shingles? A. HIV B. Advanced age C. Malignancy D. Obesity E. Chronic illness
Self-Assessment Questions 1. Answer: D Immune suppression and advanced age are the two major risk factors for shingles.
Self-Assessment Questions 2. What’s the cumulative life time incidence of shingles? A. 0-10% B. 10-20% C. 20-30% D. 30-40% E. 40-50%
Self-Assessment Questions 2. Answer: B The cumulative life time incidence of shingles in the USA is between 10-20%.
Self-Assessment Questions • 3. Which of the following is not a recognized complication of VZV infection? • Acute retinal necrosis • Herpes zoster ophthalmicus • Aseptic meningitis • Herpes zoster esophagitis • Herpes zoster oticus
Self-Assessment Questions 3. Answer – D. Herpes zoster esophagitis is not a recognized complication of VZV infection. All others are known complications.
Self-Assessment Questions • 4. One of your clinic patients presents with findings suggestive of possible VZV. You decide to perform a scraping of one of the lesions to send for further testing. What is the preferred test to help confirm the diagnosis? • Tzanck smear • DFA • PCR • Serologic testing • Viral culture
Self-Assessment Questions 4. Answer – B. DFA. PCR is the most sensitive method available, but it is still very expensive and not widely available. Both methods are now preferable to the old standard Tzanck smear. Culture is difficult and impractical. It may take up to 3 wks for results.
5. What treatment should be used for uncomplicated • herpes zoster? • Steroids alone • IV acyclovir • Foscarnet • Acyclovir and steroids • VZV Vaccine Self-Assessment Questions
5. Answer D. Out of the list of possible answers, an antiviral such as acyclovir and steroids would be the best for treatment of an episode of herpes zoster. Steroids should not be used alone. Foscarnet is reserved for acyclovir-resistant zoster. VZV vaccine would be good for prevention of future episodes of shingles. Self-Assessment Questions
6. What has been shown to be useful for pain control • in herpes zoster? • NSAIDs • Steroid cream • Short-acting opioids • Tricyclic antidepressants • C and D Self-Assessment Questions
6. Answer E. Opioids, either short-acting such as percocet or vicodin or long-acting such as a transdermal fentanyl patch are useful. Topical lidocaine patches have also been shown to be useful. NSAIDs or steroid creams have not been shown to be helpful with pain control. Self-Assessment Questions
References • Albrecht, M.A. Clinical features of varicella-zoster virus infection: Herpes zoster, UptoDate, 2005. • Albrecht, M.A., Treatment and Prevention of Herpes Zoster, UpToDate, 2005. • Gnann, J.W., Whitley, R.J., Clinical Practice: Herpes Zoster, NEJM, 2002, 347: 340-346. • Kost, R.G., Straus, S.E., Postherpetic Neuralgia – Pathogenesis, Treatment, and Prevention, • NEJM, 1996, 335: 32-42. • Oxman, M.N. et al., A Vaccine to Prevent Herpes Zoster and Postherpetic Neuralgia in • Older Adults, NEJM, 2005, 352: 2271-2284. • The Center for Shingles and Postherpetic Neuralgia. (http://shingles.mgh.harvard.edu/lab_diagnosis.htm)