Comprehensive Guide to Lumbar Puncture Procedure
300 likes | 789 Views
Learn about the indications, contraindications, techniques, and equipment required for performing a lumbar puncture, as well as potential complications and their management. History, indications, contraindications, equipment, procedural steps, patient positioning, manometry, and sample collection discussed.

Comprehensive Guide to Lumbar Puncture Procedure
E N D
Presentation Transcript
Lumbar Puncture Kalpesh Patel, MD Dept. of Pediatric Emergency Medicine December 6, 2006
Objectives • To learn the indications and contraindications for performing lumbar puncture • To learn lateral decubitus and sitting procedure for lumbar puncture • To learn the median and paramedian approach • To review complications that can occur with lumbar puncture, their precautions and treatments
History • CSF first examined in 19th century using primitive techniques (sharpened bird quills) • Modern technique first performed by Quincke in 1890 on a small child and has changed little since then
Indications • To obtain CSF for the diagnosis of: • Meningitis • Meningoencephalitis • Subarachnoid hemorrhage • Malignancy – diagnosis and treatment • Pseudotumor Cerebri • Other neurologic syndromes
Contraindications • Unstable patient with cardiovascular or respiratory instability • Localized skin/soft tissue infection over puncture site • Evidence of unstable bleeding disorder • Platelets < 50,000 or clotting factor deficiency
Contraindications • Increased intracranial pressure • Head CT before study if focal neurologic findings present to rule out impending cerebral mass herniation • Normal CT does not preclude intracranial HTN • Do not delay antibiotics to obtain imaging studies when bacterial meningitis is strongly suspected • Neurologic deterioration can occur if LP is done below the level of a complete spinal subarachnoid block • Caution in patients with Chiari malformations
Equipment • Most CSF trays come with: • Anesthetic such as: • Topical - EMLA, Elamax, Zylocaine cream • Lidocaine 1% with 25 gauge needle and syringe • Povidone-iodine solution & sponge wand • Drapes, gauze, and bandages • Manometer, stopcock and tubing in non-infant kits
Equipment • Spinal needle, usually 22 gauge • 1.5 in for < 1 yr • 2.5 in for 1 year to middle childhood • 3.5 in for older children and adolescents • Larger for large adolescents • Atraumatic needles, less spinal headaches
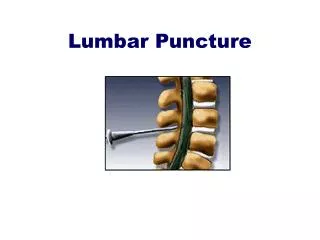
Lateral Decubitus Position • Apply topical anesthetic 30-45 min prior to procedure • Spinal cord ends at L1-L2, so sites for puncture are located at L3-L4 or L4-L5 • Restrain patient in lateral decubitus position • Maximally flex spine without compromising airway • Keep alignment of feet, knees and hips • Position head to left if right handed or vice versa
Procedure • Cleanse skin with povidone iodine from puncture site radially out to 10 cm and ALLOW TO DRY • Drape below patient and around site with fenestrated drape • Anesthetize with lidocaine if topical not used by: • Intradermally raising a wheal at needle insertion site • Advance needle through wheal to desired interspace • Careful not to inject into a blood vessel or spinal canal
Procedure • Insert spinal needle with stylet with bevel up to keep cutting edge parallel with nerve and ligament fibers
Procedure • Aim towards umbilicus directing needle slightly cephalad • Hold needle firmly
Procedure • A “pop” of sudden decrease in resistance indicates that ligamentum flavum and dura are punctured • Remove stylet and check for flow of spinal fluid
Procedure • If no fluid, then: • Rotate needle 90° • Reinsert stylet and advance needle slowly checking frequently for CSF • Jugular vein compression can increase CSF pressure in low flow situations • If bony resistance is felt immediately then you are not in the spinal interspace • If bony resistance is felt deeply, then withdraw needle to the skin surface and redirect more cephalad and increase patient flexion • If bloody fluid that does not clear or that clots results, then withdraw needle and reattempt at a different interspace
Manometry • When CSF flows, attach manometer to obtain opening pressure if desired • Pressure can only be accurately measured in lateral decubitus position and in the relaxed patient • Attach manometer with a 3-way stopcock when free flow of CSF is obtained • Read column when highest level is achieved and respiratory variation is noted
Procedure • Collect 1ml of CSF in each of 3 vials for: • Tube 1: culture & gram stain • Tube 2: glucose, protein • Tube 3: cell count & differential • and extra CSF if desired for other lab tests • Check closing pressure with manometer, if desired • Reinsert stylet and remove needle in one quick motion • Cleanse back and cover puncture site
Sitting Position • Restrain infant in the seated position with maximal spinal flexion • Hold infant’s hands between flexed legs with one hand and flex head with the other hand • Drape patient below buttocks and fenestrated drape opening over puncture site • Insert needle so bevel is parallel to spinal cord (Bevel left or right) • Cannot measure pressure accurately in this position
Paramedian (Lateral) Approach • Use for patients who have calcifications from repeated LPs or anatomic abnormalities • Needle passes through erector spinae muscles, and ligamentum flavum • Bypasses supraspinal and interspinal ligaments • Less incidence of spinal headache
Complications • Headache • Uncommon in < 10 y/o • Apnea (central or obstructive) • Back pain • Occasionally with short-lived referred limp • Disc herniation if needle advanced too far • Bleeding or fluid leak around spinal cord • Infection, pain, hematoma • Subarachnoid epidermal cyst • Ocular muscle palsy (transient) • Nerve Trauma • Brainstem herniation
Spinal Headache • Most common complication • Risk factors: female, age 18-30, lower BMI, hx of HA, prior spinal HA • Bilateral HA, improves when supine • Can last hours to weeks • Supine position for at least 2 hours • Hydration • Caffeine either PO or IV • Epidural blood patch
Spinal Headache Prevention • Can avoid by: • Passing needle bevel parallel to longitudinal fibers of dura • Replacing stylet before removing needle • Using small diameter needles • Using atraumatic needles • Bed rest or PO intake after LP does not reduce incidence of headache
Nerve Root Trauma/Irritation • Can feel electric shocks or dysesthesias • Back pain can persist for months • Consider disc herniation • Rarely permanent • Withdraw needle immediately • If pain or motor weakness persists, start corticosteroids • Electromyogram/nerve conduction velocity studies should be scheduled if pain persists
Herniation • Manifests initially as altered mental status, followed by cranial nerve abnormalities and Cushing triad • May be rapidly fatal. • Immediately remove needle and raise the head of bed to 30-45° improve venous return from the brain. • Mannitol or 3% Saline • Intubate patient and hyperventilate • Emergent neurosurgical consult
Epidermal Inclusion Cyst • Very rare due to use of stylet • Occurs when a core of skin is driven into spinal or paraspinal space with hollow needle • Do not remove stylet until through the skin
Failure of Procedure • If sample of CSF is critical several alternatives are available: • Have someone else try • Anesthesia • Neurology • Bedside ultrasound for difficult LPs • Radiographic guided procedure • Fluoroscopy • Ultrasound • CT • Cisterna Magna tap
Bibliography • Fleisher GR, Ludwig S, Henretig FM. Textbook of Pediatric Emergency Medicine Fifth Edition. Lippincott Williams & Wilkins 2006. p201-212. • Levin DL, Morriss FC. Essentials of Pediatric Intensive Care Second Edition. Churchill Livingstone 1997. p369-370,411-412. • Robertson J, Shilkofski N. The Harriet Lane Handbook Seventeenth Edition. Elsevier Mosby. 2005. p86-88. • King C, Henretig Fred. Pediatric Emergency Procedures. Lippincott Williams & Wilkins 2000. p 124-128. • Straus SE, Thorpe KE, Holroyd-Leduc J. How do I perform a lumbar puncture and analyze the results to diagnose bacterial meningitis? JAMA. 2006 Oct 25;296(16):2012-22. • Peterson MA, Abele J. Bedside ultrasound for difficult lumbar puncture. J Emerg Med. 2005 Feb;28(2):197-200. • Runza M, Pietrabissa R, Mantero S. Lumbar Dura Mater Biomechanics: Experimental Characterization and Scanning Electron Microscopy Observations. Anesthesia and Analgesia. 1999;88:1317-21. • Sucholeiki R, Waldman A. Lumbar Puncture (CSF Examination). E-medicine. 2006 http://www.emedicine.com/neuro/topic557.htm. • Walter K. Manual of Common Bedside Surgical Procedures Second Edition. Lippincott Williams & Wilkins 2000. p181-186. • Boon JM, Abrahams, PH, Meiring JH, Welch T. Lumbar Puncture: Anatomical Review of a Clinical Skill. Clinical Anatomy 2004;17:544-553 • Evans RW. Special Report: Complications of Lumbar Puncture and Their Prevention with Atraumatic Lumbar Puncture Needles. Medscape 2000. http://www.medscape.com/viewarticle/420288.