Download

1 / 27
350 likes | 660 Views
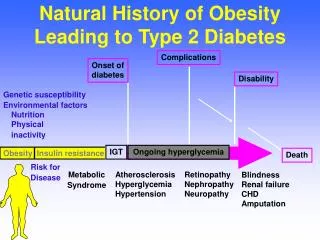
PUTATIVE ENVIRONMENTAL TRIGGER. HUMORAL AUTOANTIBODIES. (ICA, IAA, Anti-GAD 65 , IA 2 Ab, etc.). CLINICAL ONSET. Natural History of Type 1 Diabetes. CELLULAR (T CELL) AUTOIMMUNITY. LOSS OF FIRST PHASE INSULIN RESPONSE (IVGTT). BETA CELL MASS. GLUCOSE INTOLERANCE (OGTT). GENETIC

E N D
PUTATIVE ENVIRONMENTAL TRIGGER HUMORAL AUTOANTIBODIES (ICA, IAA, Anti-GAD65, IA2Ab, etc.) CLINICAL ONSET Natural History of Type 1 Diabetes CELLULAR (T CELL) AUTOIMMUNITY LOSS OF FIRST PHASE INSULIN RESPONSE (IVGTT) BETA CELL MASS GLUCOSE INTOLERANCE (OGTT) GENETIC PREDISPOSITION INSULITIS BETA CELL INJURY “PRE”-DIABETES DIABETES TIME
TrialNet International Sites • Australia • United Kingdom • Finland • Italy & Germany
Immune Tolerance Network Collaborate on Trials & Mechanistic Assays Concomitant Review of Protocols
TrialNet Goals • Explore new therapies in: • New-onset Type 1 Diabetes • Relatives “at risk” of Type 1 Diabetes • High genetic risk individuals • Further define epidemiology, natural history, and risk factors of Type 1 Diabetes
MULTIPLE ANTIBODY POSITIVE LOSS OF FIRST PHASE INSULIN RESPONSE NEWLY DIAGNOSED DIABETES Type 1 Diabetes TrialNet Studies GENETICALLY AT-RISK BETA CELL MASS GENETIC PREDISPOSITION INSULITIS BETA CELL INJURY “PRE”-DIABETES DIABETES TIME
TrialNet Prevention Trials • Relatives at Risk • Current End Point – Development of Diabetes • Genetically at Risk Relatives • End Point – Development of Autoantibodies
DPT-1 Objective To determine whether antigen based therapies (specifically, insulin) of non-diabetic relatives can delay development of Type 1 diabetes.
DPT·1 Intervention Protocols • Parenteral Insulin In Subjects with 5 year Risk of Type 1 Diabetes > 50% • Oral Insulin In Subjects with 5 year Risk of Type 1 Diabetes = 26-50%
DPT·1 Screening Results • 103,391 Relatives Screened • 97,635 Eligible Samples • 97,273 Samples Analyzed • 3480 Samples ICA+ (3.58%)
DPT-1 – Time to Diabetes By Number of Antibodies 1.0 0.9 0.8 0.7 0.6 Survival Distribution Function 0.5 P- Value< 0.001 (Log Rank Test) 0.4 Number at Risk 0.3 24151 1718 405 378 147 22297 1401 297 255 95 17049 1045 229 192 61 11807 743 163 130 40 9052 557 118 78 30 7439 457 91 49 22 6198 371 66 31 16 0 1 2 3 4 3524 199 35 14 8 0.2 0.1 0.0 0 1 2 3 4 5 6 7 8 Years Followed n = 26799 1 2 4 0 3 STRATA:
DPT-1 – Time to Diabetes ICA- vs Staging Outcome (Parenteral, Oral, Not Eligible) 1.0 0.9 ICA+ Not Eligible 0.8 0.7 0.6 Oral Insulin Trial Survival Distribution Function 0.5 P- Value< 0.001 (Log Rank Test) Parenteral Insulin Trial 0.4 Number at Risk 0.3 ICA – Subjects Not Elig Rand (Staged) Rand – Oral Rand - Parenteral 41933 879 372 339 39352 659 344 293 32410 527 283 223 24434 395 212 156 19278 285 156 97 14667 193 77 49 10631 98 35 12 5544 12 4 0.2 0.1 1 0.0 0 1 2 3 4 5 6 7 8 9 Years Followed n = 43523 Not Elig Rand (Staged) ICA – Subjects STRATA: Rand - Parenteral Rand – Oral
MULTIPLE ANTIBODY POSITIVE LOSS OF FIRST PHASE INSULIN RESPONSE NEWLY DIAGNOSED DIABETES Type 1 Diabetes TrialNet Studies GENETICALLY AT-RISK BETA CELL MASS GENETIC PREDISPOSITION INSULITIS BETA CELL INJURY “PRE”-DIABETES DIABETES TIME
C-peptide NH2 S COOH A chain S S B chain Insulin
TrialNet Intervention Trials • Recent Onset Type 1 Diabetes • Current End Point – Preservation of C-Peptide • Later Stage Type 1 Diabetes with Preserved C-Peptide • Potential End Point – Preservation of C-Peptide
Example of Mixed Meal Tolerance Test Active Rx Placebo
Changes in C-Peptide Responses During MMTT Over Time Herold et al, NEJM 2002; 346:1692
Glucagon Stimulated C-Peptide Over Time Active Rx Placebo
TrialNet Interventions • New-Onset Diabetes • Anti-CD3 (via ITN collaboration) • Mycophenolate Mofetil +/- Anti-CD25 • Anti-CD20 • Anti-CD3 + Exenatide • IL-2 plus Sirolimus – Phase 1 Safety Study • Relatives At Risk • Natural History • Oral Insulin • Beta Cell Preservation (exenatide) – pilot study • Anti-CD3 • Newborns • Nutritional : Omega-3-Fatty Acids
Other TrialNet Studies • Comparison of Mixed Meal Tolerance Test and Glucagon Stimulation Test for Stimulation of C-Peptide • Reproducibility and Validation of T-Cell Assays for Monitoring of Diabetes Intervention Trials • Collaboration with Type 1 Diabetes Genetics Consortium (T1DGC)
Key Elements of Successful Clinical Trials • Prospective • Randomized • Controlled • Statistical power • Objective endpoints • Risk/benefit to individual • Cost benefit to society
What We Need • Proven biomarkers for disease progression or improvement • Better mechanistic assays • Study designs that involve fewer subjects • Better rationale for moving potential interventions to RCTs • The courage to study interventions with potential adverse side effects