SICU Combine meeting
480 likes | 772 Views
SICU Combine meeting. 2012-4-26 è”¡å£ å¦‚. Case Presentation. 56yr, Male: CAD s/p POBAS with ICMP s/p heterotopic heart transplantation in 2004 Hypertension Gout CRI

SICU Combine meeting
E N D
Presentation Transcript
SICU Combine meeting 2012-4-26 蔡壁如
Case Presentation • 56yr, Male:CAD s/p POBAS with ICMP s/p heterotopic heart transplantation in 2004 • Hypertension • Gout • CRI • Current Medication:Burinex 1 mg/tab 1 tab BID SR Diltelan SR 120 mg/cap 1 capFolic Acid 5 mg/tab 1 tab QD PO Allopurinol 100 mg/tab 1 tab BID PO Colchicine 0.5 mg/tab 1 tab BID PO SandimmunNeoral 25 mg/cap 2 cap BID POCellCept 250 mg/cap 2 cap BID PO
ER 2012-1-25 • At ER, afebrile but SpO293% with short of breath. • EKG monitor showed intermittent VT. • Cardiac echo showed poor recipient heart with LVEF:23% • LV systolic function is normal with LVEF:61.6%. • BUN, Creand potassium was 118, 6.06 and 7.9(H9). • Under the impression of acute kidney injury, suspected rejection or infection-related
2012-1-26 start RRT • AKI Cause • Sepsis ? • Rejection ? • Both? Acute on chronic ?
問題一:重症透析的人工膜選擇 5008HF Stenotrophomonasmaltophilia 1/30, 2/8, 2/10, 2/15
Unveiling Current Controversies inAcute Kidney Injury Kellum JA, Ronco C, Vincent J- L (eds): Controversies in Acute Kidney Injury. ContribNephrol. Basel, Karger, 2011, vol 174, pp1–3
Dialyzer membranes for RRT in AKI 2012 KDIGO guideline for AKI
Hemodialysis-membrane biocompatibility and mortality of patients with dialysis-dependent acute renal failure: a Prospective randomized multicenter trial 人工膜:1.2m2
Low-Flux vs High Flux Synthetic Dialysis Membrane in Acute Renal Failure : Prospective Randomized Study • In conclusion, no significant differences were found in the results of low-flux versus high-flux synthetic membrane dialyzer treatment in patient in terms of survival rate, recovery of renal function, ……. • Low-flux synthetic polysulphone dialyzer (1.3 m2) vs High-flux synthetic AN-69(1.3m2) Artif Organs, Vol 25, No. 12, 2001
Membranes for Dialysis and Hemofiltration --- 7.3 • Management of Acute Kidney Problems • D. H. Krieter and C. Wanner. 2010 • Materials : Synthetic membrane √ • Low-flux vs High-flux • Size
High-flux vs Low-flux • The Hemodialysis (HEMO) study • not find a difference between low- and high-flux membranes Effects of high-flux hemodialysis on clinical outcomes: Results of the HEMO Study. J Am SocNephrol 2003 14:3251-3263. • MPO study ( Membrane Permeability Outcome) • High-flux benefits in DM and low serum albumin levels (< 4 g/dl) • No significant survival benefit Membrane Permeability Outcome (MPO) Study Group Effect of membrane permeability on survival of hemodialysis patients. J Am SocNephrol2009 20:645-654
No study was able to demonstrate differences in survival between low- and high-flux membranes. • Is the choice of membrane important for patients with acute renal failure requiring hemodialysis? 1995 ArtifOrgans 19:391-394. • Patient survival and renal recovery in acute renal failure: randomized comparison of cellulose acetate and polysulfone membrane dialyzers. 2000 Mayo Clin Proc 75: 1141- 1147. • Comparison of cellulose diacetateand polysulfone membranes in the outcome of acute renal failure. A prospective randomized study. 2000 NephrolDial Transplant 15:224- 230 • Low-flux versus high-flux synthetic dialysis membrane in acute renal failure: prospective randomized study. 2001 ArtifOrgans 25:946-950. • Only with respect to the recovery of renal function that a possible advantage of high- over low-flux membranes. • (2000) Patient survival and renal recovery in acute renal failure: randomized comparison of cellulose acetate and polysulfone membrane dialyzers. Mayo Clin Proc 75: 1141- 1147. • Biocompatible hemodialysis membranes for acute renal failure. 2008 Cochrane Database SystRev 23:CD005283
Modality of ARRT with Efficiency Defined Marshall MR, Golper TA:Semin Dial 24:142-148,2011
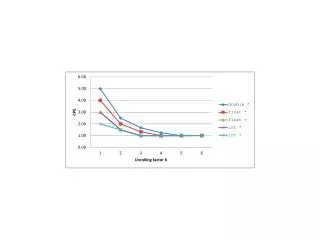
Low-Efficiency Acute Renal Replacement Therapy : Role in Acute Kidney Injury • PIRRT effect of urea disequilibrium on time concentration profiles inbound and rebound • 1.8 m2 low-flux(QB200, QD100, 12HR) 4% rebound • 1.8 m2 low-flux (QB200, QD500, 8hr) 17% rebound • High-efficiency PIRRT • Unacceptable Disequilibrium Mark R. Marshall*† and Thomas A. Golper • Seminars in Dialysis—Vol 24, No 2 (March–April) 2011 pp. 142–148
Low-Efficiency Acute Renal Replacement Therapy : Role in Acute Kidney Injury
Low-Efficiency Acute Renal Replacement Therapy : Role in Acute Kidney Injury three major ways in which solute disequilibrium affects the clinical care of patients: • ARRT dose • dialysis disequilibrium syndrome • hemodynamic instability
solute disequilibrium • Symptoms of headache, disorientation and nausea at its mildest, delirium, myoclonus ⁄ seizures and coma at its most severe. • The pathogenesis is incompletely understood although it is clearly attributable to cerebral edema from water influx as the final common pathway Ronco C, Bellomo R, KellumJ. Critical Care Nephrology. 2009:1079–1083
Low-Efficiency Acute Renal Replacement Therapy : Role in Acute Kidney Injury • Prosaic Use of Lower-Efficiency ARRT • Low-flux membrane • Lower-efficiency
Case Presentation • 52yrs, AMI with ventricular septal rupture status post repairmen of ventricular septum on 2012/01/07, • Tachypnea and agitation were noted around 8PM on 2/19, and desaturation to 90% was found. CXR showed pulmonary edema, r/o pneumonia, and BW gain>7Kg , metabolic acidosis with dopamine infusion, he was transferred to ICU. And start CRRT. • 2/20 5008HF(standard setting), BUN/Cre:283/5.79 2/23 BUN/Cre :33/1.83 • solute disequilibrium ??? • 停止透析:2012/3/4
Case Presentation • 35yrs, DCMP with congestive heart failure and lung edema s/p ECMO support(2012/3/22), s/p LVAD support (2012/03/26) • 3/28 septic shock start RRT (SLED 2hr due to BUN/Cre:174/4.91, prevent disequilibrium?) • 3/28 night profound acidosis 5008HF • 3/29 Expired
超過濾係數 Ultrafiltration Coefficient • Low (Standard) Flux • UFcoefficient 2-9 ml/mmHg/hour • Intermediate Flux • UFcoefficient 10-19 ml/mmHg/hour • High Flux • UFcoefficient 20-80 ml/mmHg/hour • 水份的移除 (Hydraulic Permeability) 超過濾係數Kuf • (ml/mmHg/hour)
Categories for HD membranes Vicken J. Membranes in Haemodialysis in;Peinemann KV, Pereira Nunes SP, (eds) Membranes for Life Sciences. Wiley Co, 2007;1-48.
血液透析器設計理念 血液過濾器設計理念 血液透析過濾器 for SLEDD-f
血液透析器 for IHD Chronic Filter 200 µm 40 µm
血液透析器設計理念 血液過濾器設計理念 血液透析過濾器 for SLEDD-f
“理想的" 血液過濾(Hemofilter) • 具高生物相容性 • 具良好的中大分子篩濾與清除效果 • 抗凝劑需要量越低越好 • 最少可連續使用24小時
“理想的" 血液過濾器 • Function • Membrane permeability • Diffusion Low flux and High flux • Convention High flux • Filter and Fiber Geometry • Adapted for low blood flow • Large ID:short • Biocompatibility
血液過濾器 – 中空纖維特性 Membrane geometry adapted to special needs in CRRT • Decreased wall thickness • increased diffusive clearance • Increased inner lumen • less shear-stress • lower thrombogenicity • lower heparin need Acute Filter 35 µm 220 µm
血液透析器設計理念 血液過濾器設計理念 血液透析過濾器 for SLEDD-f
S i e v i n g C o e f f i c i e n t 1 , 0 0 , 8 S t a n d a r d m e m b r a n e P o l y s u l f o n e Ultra - F l u x K i d n e y 0 , 6 0 , 4 0 , 2 0 100 1000 100000 10000 10 I n u l i n ß 2 - M A l b u m i n V i t . B U r e a C r e a t i n i n e 1 2 M o l e c u l a r W e i g h t [ D a l t o n ] high-flux dialyzer is required to SLEDD-f • A high-flux dialyser is required to perform SLEDD-f • A dialysis membrane with high hydraulic permeability, high solute permeability and large surface exchange • Moderate transmembrane pressures (< 300mmHg) • Simultaneously avoid or minimal albumin loss • Highly biocompatible membrane is particular importance The cut off of the membrane is ~ 30.000 Dalton.
Membranes for Dialysis and Hemofiltration --- 7.3 Dialysis membranes should have: • high diffusive and convective clearances for the removal of a wide range of toxins. • the best possible biocompatibility to avoid undesirable interactions with blood components • adequate hydraulic permeability for use in intermittent or continuous renal replacement therapy modes • the highest pyrogenretention capability for the use with non-ultrapure dialysate.
Membrane Size • 早期: 1.2 m2 • 近期: 1.4 ~ 1.8 m2
SICU Dialysis method 選一種人工腎臟:兼顧PIRRT and IHD ? CRRT:1.4 m2 AV-600
AN-69 : Bradykininrelease syndrome