Acute Cough
Acute Cough. Definitions of Lower Respiratory Tract Infections (LRTI), ranging in severity: Acute bronchitis - an acute respiratory tract infection in which cough, with or without phlegm, is the predominant symptom

Acute Cough
E N D
Presentation Transcript
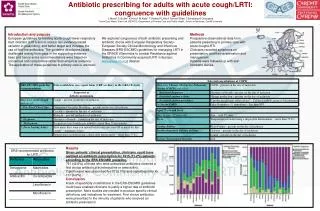
Acute Cough Definitions of Lower Respiratory Tract Infections (LRTI), ranging in severity: • Acute bronchitis - an acute respiratory tract infection in which cough, with or without phlegm, is the predominant symptom • LRTI - an acute respiratory tract infection with cough, with or without phlegm, plus 1 other clinical sign plus 1 constitutional symptom • CAP - acute pneumonia (infection of lung parenchyma) acquired in the community rather than in hospital
LRTI in the communityFeldman C. Primary Care Resp J 2004; 13: 159–66 Pneumonia diagnosed in community: 100 Pneumonia admitted: 20 ITU: 1–2 Die: 1–2 Antibiotics Prescribed 2,000 Consultations 8,000 Acute LRTI in community 24,000
Who is likely to get CAP?Clinical Evidence. Loeb M. Search date April 2005 • Affects about 1.2% people per year, particularly during winter and at the extremes of age • Annual incidence: < 1 year old 3–5% 15–45 years 0.1–0.5% 60–70 years 1–2% 71–85 years 5–10 % • 60–75% in UK caused by Strep pneumoniae (but a pathogen is identified only about 50% of the time) • Mortality 13.7%, (Range: 5.1% for ambulant people to 36.5% for people requiring intensive care) Some Risk Factors : Alcoholism, Asthma, Immunosuppression, Lung or Heart Disease, Institutionalisation
Factors: Absence of asthma • Temp > 37.8 Heart rate > 100 • Decreased breath sounds Crackles If prevalence of pneumonia =5% (the average 71–85 year old)… No. of factors present Post test probability of pneumonia 0 <1% 1 1% 2 3% 3 10% 4 25% 5 50% Clinical Prediction tools for diagnosis of CAPHeckerling PS, et al. Ann Intern Med 1990; 113: 664–70
Some issues from the BTS Pneumonia Guidelines & UpdateBTS website 30.4.04 • Routine use of urine legionella antigen testing in more severe cases • Severity assessment using CRB + age > 65years: C – new mental confusion R – respiratory rate ≥ 30/min B – blood pressure <90mmHg systolic and / or ≤ 60mmHg diastolic • score 0–1 = low risk of death, no admission • score 1 or 2 = Increased risk of death and admission should be considered, especially at score 2 • score 3 or more = High risk of death, urgent admission required Additional adverse prognostic features • Pulse oximetry - SaO2 <92% • Bilateral or multiple involvement on chest x-ray
Role of Antibiotics CAP: Antibiotics should be prescribed (Clinical Evidence. Loeb M Search Date April 2005) Acute Bronchitis : (8–23% viral) Antibiotics appear to have a modest beneficial effect in patients who are diagnosed with acute bronchitis. The magnitude of this benefit, however, needs to be considered in the broader context of potential side effects, medicalisation of a self-limiting condition, increased resistance to respiratory pathogens and cost of antibiotic treatment. (Cochrane. Fahey et al. Issue 4 2006)
Managing Acute cough (Less severe LRTI) • Delayed prescription? This tactic has been shown to be effective in acute cough. It reduced overall antibiotic consumption and did not alter cough duration or other patient outcomes (Little P, et al. JAMA 2005;293:3029–35) • Patient Information Leaflet (PIL)? The use of a PIL has been shown to be effective in reducing the number of re attendances at the surgery (MacFarlane JT et al. BJGP 1997;47:719–22) Other Treatments: • No evidence for beta-2 agonists but proven harms (Cochrane. Smucney J, et al. Issue 4 2006) • Insufficient data to assess effectiveness of cough medicines (Schroeder and Fahey. BMJ 2002:324:1–6)
Summary • The relatively well with a cough are likely to do well on most occasions without antibiotics, and may come back less in the future if given a leaflet • The more objective signs are present, the more likely the diagnosis of pneumonia is, and the greater the need for antibiotics / CXR / admission • So…. • Assess the personal characteristics of the person with a cough (age, co-morbidities) • Assess the physical signs to decide whether those increase the probability of pneumonia • Assess the severity of those signs, including SaO2 • And then agree management plan.