Download
1 / 9

E N D
Nilotinib versus Imatinib for the Treatment of Patients with Newly Diagnosed Chronic Phase, Philadelphia Chromosome-Positive, Chronic Myeloid Leukaemia: 24-Month Minimum Follow-Up of the Phase 3 Randomised ENESTnd Trial1Comparison of Nilotinib and Imatinib in Patients (pts) with Newly Diagnosed Chronic Myeloid Leukemia in Chronic Phase (CML-CP): ENESTnd 24-Month Follow-Up2 1Kantarjian HM et al.Lancet Oncol 2011;12:841-51. 2Larson RA et al.Proc ASCO 2011;Abstract 6511.
ENESTnd: Phase III Trial Design RANDOMIZED* Nilotinib 300 mg BID (n = 282) • N = 846 • 217 centers • 35 countries Nilotinib 400 mg BID (n = 281) Imatinib 400 mg QD (n = 283) Follow-up5 years * Stratification by Sokal risk score Primary endpoint: Major molecular response (MMR) at 24 months Secondary endpoints: Complete cytogenetic response (CCyR), time to MMR and CCyR, event-free survival (EFS), progression-free survival (PFS), time to accelerated phase/blast crisis (AP/BC), overall survival (OS) Kantarjian HM et al. Lancet Oncol 2011;12:841-51.
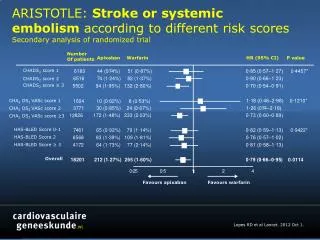
ENESTnd: Outcomes — First 24 Months Kantarjian HM et al. Lancet Oncol 2011;12:841-51.
Kantarjian HM et al. Lancet Oncol 2011;12:841-51. Cumulative Incidence of MMR* * ITT population used for all efficacy analyses
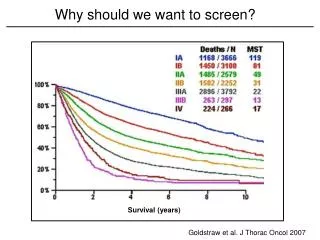
Larson RA et al. Proc ASCO 2011;Abstract 6511. MMR Rates by 24 Months According to Sokal Risk* p = .003 p < .0001 p = .002 p < .0001 80 p = .0008 74 74 73 p = .002 67 70 65 56 60 53 50 44 % MMR 40 32 30 20 10 0 n = 103 103 104 101 100 101 78 78 78 Low Intermediate High Nilotinib 300 mg BID Nilotinib 400 mg BID Imatinib 400 mg QD * p values are provided for descriptive purposes only and are not adjusted for multiple comparisons Data cutoff: 20 Aug 2010
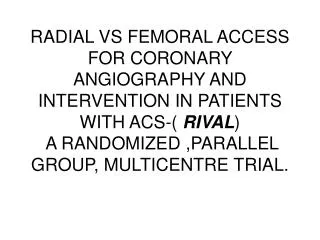
Larson RA et al. Proc ASCO 2011;Abstract 6511. Progression to Accelerated Phase/Blast Crisis on Treatment* p = .0003 p = .0089 p = .0059 17 18 p = .0196 16 14 12 12 Number of patients 10 8 5 6 3 4 2 2 2 0.7% 1.1% 4.2% 0.7% 1.8% 6.0% 0 Including clonal evolution Nilotinib 300 mg BID Nilotinib 400 mg BID Imatinib 400 mg QD * Defined as progression to AP/BC or death due to CML while on treatment Data cutoff: 20 Aug 2010
ENESTnd: Adverse Events(24-Month Follow-Up) No patient had a QT interval corrected for heart rate of more than 500 msec. Kantarjian HM et al. Lancet Oncol 2011;12:841-51.
Author Conclusions • Compared with imatinib, nilotinib continues to demonstrate: • Superior MMR, CMR and CMR • Significantly fewer progressions to AP/BC on treatment • Nilotinib demonstrated significantly higher MMR rates compared with imatinib in all Sokal risk groups. • Safety and efficacy of nilotinib and imatinib in elderly patients was comparable to younger patients (data not shown). • Nilotinib at both doses was generally well tolerated, and fewer adverse events led to discontinuation in the nilotinib 300 mg BID arm. • Longer follow-up confirms the superiority of nilotinib over imatinib for the treatment of patients with newly diagnosed CML-CP. Kantarjian HM et al. Lancet Oncol 2011;12:841-51; Larson RA et al. Proc ASCO 2011;Abstract 6511.
Investigator Commentary: The Results from the 24-Month Update of the ENESTnd Trial This was an update of an important data set previously published in The New England Journal of Medicine last year. The primary endpoint for the ENESTnd trial was major molecular response at 12 months, and the primary endpoint was clearly metwith both 300 mg and 400 mg of nilotinib twice a day. One issue, however, was that the gold standard is achieving a complete cytogenetic response in terms of long-term survival by 18 months. Now we have the 18-month follow-up and the complete cytogenetic response that was presented at ASH 2010 and then updated to 24 months at ASCO 2011. The authors reported that the complete cytogenetic response in the nilotinib arms was 87% and 85% versus only 77% with imatinib, and this was statistically significant. We are continuing to see improvement with the second-generation tyrosine kinase inhibitor used up front. Another aspect first reported in the NEJM paper that is clearly a clinically relevant endpoint is that the incidence of progression to accelerated or blast phase was lower. That finding held true with longer follow-up. This is clearly relevant because having patients develop accelerated phase or blast crisis is not good. Susan M O’Brien, MD