Download
1 / 22
230 likes | 637 Views
Chemotherapy-induced nausea and vomiting. By Alan O’Kane Specialist Pharmacist Oncology and Aseptic Ninewells Hospital. Chemotherapy-induced nausea and vomiting. Most feared side-effect May be more distressing than future concerns of life expectancy

E N D
Chemotherapy-induced nauseaand vomiting By Alan O’Kane Specialist Pharmacist Oncology and Aseptic Ninewells Hospital
Chemotherapy-induced nausea and vomiting • Most feared side-effect • May be more distressing than future concerns of life expectancy • Medical complications: dehydration, electrolyte imbalance, risk of aspiration pneumonia • Many treatments palliative intent = maintain QOL • Effective management of N + V is essential
High Risk in nearly all patients (>90%) Moderate Risk in 30-90% of patients Low Risk in 10-30% of patients Minimal Risk in less than 10% of patients. Emetogenic Risk categories for chemotherapy in untreated patients (See Figure 1) Primary Risk Factor
Patient risk factors • Age <50 years • Female • Alcohol intake • Prone to N +V
Substance P GABA Serotonin Nausea Acetylcholine Dopamine Vomiting Histamine ??????? Cannabinoid
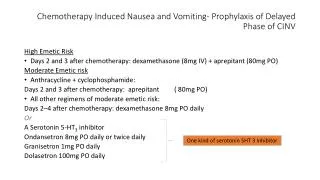
Categories of CINV • Acute - within 24 hours of chemotherapy • Delayed - 24 hours to 7 days post chemo • The most effective way of controlling CINV is to prevent symptoms of acute and delayed CINV by using a combination of an NK1 antagonist, 5HT3 antagonist and dexamethasone.
Anatomy of CINV • Brainstem vomiting enter1,2 • Area postrema • Chemoreceptor trigger zone (CTZ) • Nucleus tractus solitarius • Dorsal motor nucleus of the vagus nerve • Substance P/neurokinin 1 (NK1)receptors1 • Serotonin/5-HT3 receptors1 • GI vagal afferent nerve fibers1 • Serotonin/5-HT3 receptors • Substance P/NK1 receptors 1. Hesketh PJ et al. Eur J Cancer. 2003;39(8):1074–1080. 2. Grunberg SM, Hesketh PJ. N Engl J Med. 1993;329(24):1790–1796. Illustration by Kirk Moldoff.
Proposed pathways for CINV • CTZ activation • Blood • Cerebrospinal fluid Activated vomiting center Chemotherapy Increased afferent input to the CTZ and vomiting center Increased efferent output to target organs resulting in emesis • Cell damage • Release of neuroactive agents • Vagal activation Berger AM, Clark-Snow RA. In: DeVita VT Jr et al. 7th ed. Cancer: Principles & Practice of Oncology. Lippincott Williams & Wilkins; 2005:2515–2523. Illustration by Kirk Moldoff.
Serotonin and 5HT3 receptor pathway • Introduction of 5-HT3 receptor antagonists offered an improved treatment option.2 • Effective in acute vomiting; very limited efficacy for delayed events • Primary mechanism of action appears to be peripheral.2 1. Berger AM, Clark-Snow RA. In: DeVita VT Jr et al. 7th ed. Cancer: Principles & Practice of Oncology. Lippincott Williams & Wilkins; 2005:2515–2523. 2. Hesketh PJ et al. Eur J Cancer. 2003;39(8):1074–1080.
Substance P and NK1 receptor pathway • Substance P relays noxious sensory information to the brain • High density of substance P/NK1 receptors located in brain. • NK1 receptor blockade effective for delayed vomiting: • Less effective for acute vomiting: needs a 5HT3 antagonist • Less effective for nausea: needs dexamethasone
NK1 antagonists • Aprepitant 125mg 1 hour before chemotherapy on Day 1, 80mg Day 2 and Day 3 • SMC approved for cisplatin containing regimens (other regimens??) • Some interactions: clinical significance
5HT3 Antagonists • Block release of serotonin release from enterochromaffin cells in GI tract • Most effective for acute vomiting • All equally effective e.g ondansetron/granisetron (?palonesetron) • Best given as a stat dose pre-chemo • Oral and IV equally effective • Side effects: constipation, abdominal spasms, headaches
Multi-Association of Supportive Cancer Care (MASCC) (See Handout)
Dexamethasone • M.O.A not fully understood. • Very effective for nausea, acute and delayed vomiting • Acute: pre-dose before chemo • Delayed: 2-4 days after • Side effects: heartburn/indigestion, agitation, hiccups, abnormal BM’s (all manageable in most instances)
Anticipatory N + V • Conditional response • Sights and smells • Involves higher cortical centres of brain • Occurs in 30% of patients • Lorazepam is an effective treatment
Other situations… • Breakthrough symptoms - N + V in spite of optimal preventative treatment. • Rescue therapy - Treatment of breakthrough symptoms • Refractory - CINV recurs in subsequent cycles of therapy when all previous preventative and rescue treatments have failed.
Breakthrough symptoms- which anti-emetic? • Less well-conducted trials available to guide treatment decisions. • Diagnosis of the cause of nausea and vomiting is crucial for deciding on which anti-emetic to use. • Key questions- when did symptoms start? when was last dose of chemo/XRT? When did steroid course stop? Nausea related to smells/taste of food? How many vomiting episodes? VAS to assess nausea? Appetite/food and fluid intake? • The only evidence available to rescue patients who have CINV is with the use of a D2 antagonist e.g. metoclopramide or a 5HT3 antagonist such as ondansetron. • Consider the side-effect profile of each anti-emetic. There may be more than one cause of nausea and vomiting therefore do not prescribe an anti-emetic that may worsen symptoms e.g. ondansetron and cyclizine may constipate- avoid if constipation and nausea present- use metoclopramide instead. • Severe cases- consider syringe driver for 48 hours then review. • Domperidone is supplied at a dose of 20mg qds with the majority of chemotherapy regimens. Consider if you want to add or substitute. If patient feels ineffective- consider compliance in view of low confidence in medicine.
Effective control • Give appropriate antiemetic medicines before chemo and after at correct dose, route, frequency, duration and timing • Start “prophylaxis” Cycle 1 and then throughout • “Breakthrough symptoms”- diagnosis cause and chose anti-emetic wisely (consider anti-emetic choice, dose, frequency, duration and side effect profile). • Counsel patient on diet when feeling sick or vomiting- importance of small amounts of food frequently (5-6 meals instead of 3), plenty fluid, eat easy to swallow foods with minimal smell e.g. clear broth, white toast, yoghurt, custard, crackers.