Download
1 / 111
1.13k likes | 1.7k Views
ACID BASE DISORDERS AND ARTERIAL BLOOD GAS ANALYSIS. Dr chandan bansal. introduction. Endogenous acid production. Normally when food is metabolised , two types of acids are added to the ECF.

E N D
ACID BASE DISORDERS AND ARTERIAL BLOOD GAS ANALYSIS Drchandanbansal
Endogenous acid production Normally when food is metabolised, two types of acids are added to the ECF. • Volatile acid in the form of carbonic acid, which determines level of CO2 in the blood (PaCO2) and is excreted by lungs. About 22,000 mEq volatile acid is produced daily. • Nonvolatile acid ( like sulphuric and phosphoric acids) are produced by dietary and endogenous protein catabolism, roughly at the rate of 1mEq/kg. they are excreted by the kidney.
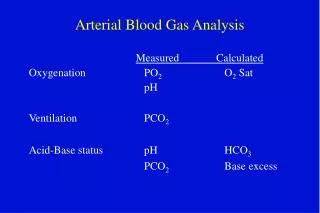
Regulation of acid base • The regulation of the pH in a narrow range is the function of buffers, lungs and kidneys. • The henderson-hasselbalch equation describes the correlation of metabolic and respiratory regulations, which maintains pH. pH = 6.1 + log HCO3 / 0.3 x PaCO2 = pK + kidney/lung
Buffers Buffers are chemical systems, which either releases or accepts H+. So buffers minimize change in pH induced by an acid or base load and provides immediate defence. Most important buffers are • bicarbonate, • phosphate, • proteins, • haemoglobin, and • bone bicarbonate.
Respiratory regulations • By excreting volatile acids, lung regulates PaCO2. • Normally CO2 production and excretion are matched, which maintains CO2 at 40mm of Hg. • When rate of CO2 production increases it will stimulate PaCO2 sensitive chemoreceptors at the central medulla with resultant rise in rate and depth of breathing. This hyperventilation will maintain PaCO2 to normal range. • Respiratory regulation acts rapidly ( in seconds to minutes) and has double buffering power as compared to the chemical buffers.
Renal regulations • The role of kidney is to maintain plasma HCO3 concentration and thereby pH regulation. It has the most powerful buffering system, which starts within hours and takes 5-6 days for peak level. • The kidney regulates HCO3 by excreting nonvolatile fixed acids by following three mechanisms. • Excretion of H+ ions by tubular secretions. • Reabsorption of the filtered bicarbonate ions • Production of new HCO3 ions.
ANION GAP METABOLIC ACIDOSIS Check anion gap (AG) = Na - (Cl+ HCO3) unmeasured cations - unmeasured anions. • expected AG is [albumin] x 2.5 (ie, 10 if albumin is 4 g/dL, 7.5 if albumin is 3 g/dL) • Increase in AG is because of increase in unmeasured anions such as organic acids, phosphates, sulfates. • Decrease in AG is because of decrease in albumin or increase in unmeasured cations (Ca, Mg, K, Li, bromine, immunoglobulin)
Metabolic Acidosis……. + additional disorders Equivalent rise of AG and Fall of HCO3…… ….Pure Anion Gap Metabolic Acidosis Discrepancy…….. in rise & fall + Non AG M acidosis, + M Alkalosis
PURE Anion Gap Acidosis + • Delta gap = HCO3+ ∆ AG • Delta Gap = 24….Pure AG acidosis • < 24 = non AG acidosis (+ AG M Acidosis) • > 24 = metabolic alkalosis (+ AG M Acidosis)
Delta Gap = 24 ……AG met Acidosis < 24 ….. + Non AG Mac > 24 ….. + Meta. Alkalosis N-HCO3 = 24, N-Anion Gap = 12 Delta Gap = HCO3 + ∆ AG • e.g. if HCO3 = 12, AG = 30, ∆ AG = 18 Delta Gap = 12 + 18 = 30 > 24 ….AG + metabolic Alkalosis N-HCO3 = 24, N-Anion Gap = 12 Delta Gap = HCO3 + ∆ AG e.g. if HCO3 = 12, AG = 20, ∆ AG = 8 Delta Gap = 12 + 8 = 20, < 24 …AG + Non AG metabolic Acidosis N-HCO3 = 24, N-Anion Gap = 12 Delta Gap = HCO3 + ∆AG e.g. if HCO3= 12, AG = 24, ∆ AG = 12 Delta gap = 12 + 12 = 24 ….Pure AG Metabolic Acidosis
Workup for AG metabolic acidosis • CHECK for ketonuria (dipstick acetoacetate) or plasma Beta Hydroxybutyrate. If negative for ketones, CHECK renal function, lactate, toxin screen, and osmolal gap. Osmolal gap (OG) = measured osmoles - calculated osmoles Caldosmoles = (2 xNa) + (glucose/18) + (BUN/2.8 or urea/5.6) (calculate + [EtOH/4.6] if have EtOH level and want to test if other ingestions) OG >10 suggests ingestion.
Workup for non-AG metabolic acidosis • Evaluate history for causes. • Check urine anion gap (UAG) = (UNa + Uk) – Ucl • UAG = unmeasured anions - unmeasured cations; • As NH4+ is primary unmeasured cation, UAG is indirect assay for renal NH4+ excretion. • Negative UAG is increased renal NH4+ excretion i.e. appropriate renal response to acidemia. Ddx: GI causes, type II RTA, ingestions or dilutional • Positive UAG is failure of kidneys to secrete NH4+ . Ddx: type I or IV RTA, early renal failure • plasma K+usually decreased in type I and increased in type IV RTA. • UAG evaluation assumes Patient not volume depleted (UNa >25) & w/o AG metabolic acidosis.
Renal tubular acidoses (RTAs) Proximal (Type II): decreased proximal reabsorption of HCO3- • Primary • (Fanconi’s syndrome, decreased proximal reabsorption of HCO3-, PO4, glucose, amino acids), • paraprotein(multiple myeloma, amyloidosis), • medicines (acetazolamide, heavy metals, ifosfamide), • renal transplant, decreased Vit D, NRTIs
Distal (Type I) defective distal H+secretion • Primary • autoimmune (Sjögren’s, RA), • nephrocalcinosis, • medicines (amphotericin B, Lithium, ifosfamide) • Normally associated with decreased K+ ; if associated with increased K+ then etiology may be sickle cell, obstruction, SLE, renal transplant.
Type IV RTA Increased K+ , decreased NH3 synthesis/delivery, decreased urine acid carrying capacity • decreased renin: diabetic nephropathy, NSAIDs, chronic interstitial nephritis, HIV • normal renin, decreased aldosterone synthesis: primary adrenal disorders, ACEI, ARBs, heparin • Decreased response to aldosterone : meds(K-sparing diuretics,TMP-SMX, pentamidine, calcineurininhibitors tubulointerstitialdisease: sickle cell, SLE, amyloid, diabetes.
Treatment of severe metabolic acidoses (pH < 7.2) • DKA: insulin & IVF;AKA: dextrose, IVF, replete K, Mg, PO4 as needed. • Lactic acidosis: treat underlying condition, avoid vasoconstrictors • Renal failure: hemodialysis • Methanol & ethylene glycol: early fomepizole, vit. B6 (ethylene glycol), folate , hemodialysis (especially if late presentation) • Alkali therapy: NaHCO3 to get serum HCO3 > 8 and pH > 7.2 .
Introduction • Saline-responsiveetiologies require initiating event and maintenance factors, whereas • Saline-resistantetiologies develop from various causes. Initiating event • loss of H+from GI tract or kidneys. • exogenous alkali. • contraction alkalosis: diuresis → excretion of HCO3-poor fluid → extracellular fluid “contracts” around fixed amount of HCO3 → ↑HCO3 concentration • Post hypercapnia: respiratory acidosis → renal compensation with HCO3 retention; rapid correction of respiratory disorder (e.g., with intubation) → transient excess HCO3
Maintenance factors • volume depletion → ↑ proximal reabsorption of NaHCO3 and ↑ aldosterone. • Hyperaldosteronism(either 10or 20 ) → distal Na reabsorption in exchange for K+ and H+excretion (and consequent HCO3 retention). • Hypokalaemia→ transcellular K+ / H+exchange; intracellular acidosis in renal proximal tubular cells promotes bicarbonate reabsorption and ammonia genesis.
Workup • Check volume status and UCl. • Ucl < 20 mEq/L → saline-responsive • Ucl > 20 mEq/L → saline-resistant (unless currently receiving diuretics) • (UNaunreliable determinant of volume status as alkalemia→ ↑HCO3 excretion →↑ Na excretion; negatively charged HCO3 “drags” Na along) • If Ucl > 20 and volume replete, ✓ blood pressure
Treatment of severe metabolic alkalosis (pH >7.6) • If volume depletion: d/c diuretics and correct volume deficit with isotonic saline. • If cardiopulmonary disease precludes hydration, can use KCl, acetazolamide. • If NGT drainage that cannot be d/c: PPI • Hyperaldosteronism: treat underlying condition
Respiratory Acidosis Reduced Pulmonary Clearance of CO2 • Compensation: • Acute: 12 - 24 hrs. • No time for renal comp. Tissues regenarate HCO3- • rare to see HCO3- above 30mEq/L • Chronic: 24 - 36 hrs. • Stimulates renal excretion of H+ and resorption and synthesis of HCO3- and returns pH towards normal • Mixed: acute on chronic • Blood pH would be lower than predicted for Chronic and higher than predicted for Acute
Causes of Respiratory Acidosis • Respiratory center inhibition • drugs (sedatives, narcotics, alcohol, hypnotics) • CNS lesions (stroke, encephalitis), myxedema • Alveolar hypoventilation • Nerve damage beyond CNS • High spinal cord injury • Phrenic palsy • GuillianBarre` syndrome • Neuromuscular junction disease • myasthenia gravis • botulism, aminoglycosides
Causes of Respiratory Acidosis • Muscle Disease • myositis, myotonic dystrophy • hypokalemia, hypophosphatemia • Chest wall disorders • kyphoscoliosis • flail chest • Airway obstruction • COPD, tracheal obstruction • increased dead space
Respiratory Alkalosis • CO2 excretion exceeds production • Acute: • RBC and tissue buffers make H+ more available so HCO3- falls by 3-4mEq/l as pCO2 falls to 25mmHg. • No loss of HCO3- in urine • Chronic: • renal acid excretion is decreased • endogenously produced acid is retained. • pH normalizes by day 4
Etiology of Respiratory Alkalosis • CNS disorders • meningtis, encephalitis, trauma, hemorrhage, fever • Metabolic disorders • sepsis, hyperthyroidism, liver failure, fever, anemia • Pulmonary disorders • pneumonia, asthma,CHF, PE, restrictive diseaeses • Drugs • salicylate excess, progesterones, catechols • Pregnancy
Base excess and base deficit • Base excess is defined as the amount of strong acid that must be added to each liter of fully oxygenated blood to return the pH to 7.40 at a temperature of 37°C and a pCO2 of 40 mmHg (5.3 kPa). • A base deficit (i.e., a negative base excess) can be correspondingly defined in terms of the amount of strong base that must be added.
Contd… • Actual base excess is that present in the blood, • Standard base excess is the value when the hemoglobin is at 5 g/dl. The latter gives a better view of the base excess of the entire extracellular fluid.
Estimation Base excess beyond the reference range indicates • metabolic alkalosis if too high (more than +2 mEq/L) • metabolic acidosisif too low (less than −2 mEq/L)
Arterial sample • Draw at least 3ml. Of blood. • 22 gauge needle and glass syringe desirable. • Avoid air bubbles. • Cool to 5 degree C immediately.
Arterial puncture complications • Spasm • Intraluminal clotting • Bleeding,hematoma • Allen’s test - check for collaterals
Potential sampling errors • Air contamination: spurious increase in PO2 • Duration of exposure more important than volume of air bubble. • Expel air immediately. • Discard sample if froth present.
Potential sampling errors Venous sample: • absence of – • flash of blood on entry into vessel; • pulsations during syringe filling; • auto filling of the syringe • Venous admixture • Cross-check with pulse oximetry and clinical status • Anticoagulant effects:dilution error- drop in PCO2 > PO2 Ph usually remains unchanged
Pulse oximetry Limitations: • carboxyhemoglobin:falsely high saturation • bilirubin:falsely low saturation • melanoticskin:variable,reduced signal • poor peripheral perfusion:lowsignal, unreliable result
…To calculate A-a gradient…. • Is the baby hypoxic? • Type and severity of Hypoxia. • …Relationship of PaO2 and FiO2? • FiO2 X 5 = Expected PaO2 • …Whether PaO2 is appropriate for the given FiO2? • …Is the O2 content (CaO2) enough to prevent hypoxia?
Alveolar-arterialO2 Difference • Classify Respiratory Failure • Ventilation–perfusion mismatch • ……FiO2 dependant derivation ………..PAO2 – PaO2 = ? PAO2 = PiO2* -(PCO2/0.8) (calculated)PAO2= 150 – 1.2 (PCO2) = 150 – 1.2 40 = 150 – 50 = 100 mmHg PAO2 O2 CO2 (measured) PaO2= 90 mmHg PaO2 PAO2 – PaO2 = 10 mmHg * When FiO2 = 21 % : PiO2 = (760-45) x .21= 150 mmHg
Alveolar-arterial Difference Ventilation Failure Normal Gap PCO2 = 80 PaO2 = 45 PAO2 = 150-1.2(80) = 150-100 = 50 Oxygenation Failure Wide Gap PCO2 = 40 PaO2 = 45 PAO2 = 150 – 1.2 (40) = 150 - 50 = 100 O2 CO2 Alveolar arterial G. 50 – 45 = 5 …………….Normal A-a Alveolar – arterial G. 100 - 45 = 55 ……………….Wide A-a