Chikungunya
USAF School of Aerospace Medicine. Chikungunya. Background. Chikungunya : V iral disease ( Genus Alphavirus ; Family Togaviridae ) Transmitted by mosquitoes (Genus Aedes ) Symptoms are often severe and debilitating Fatalities are rare Past infection gives long lasting immunity


Chikungunya
E N D
Presentation Transcript
USAF School of Aerospace Medicine Chikungunya
Background • Chikungunya: • Viral disease (Genus Alphavirus; Family Togaviridae) • Transmitted by mosquitoes (Genus Aedes) • Symptoms are often severe and debilitating • Fatalities are rare • Past infection gives long lasting immunity • At risk individuals: • Anyone who has not previously been infected by the virus • Outbreak attack rates of 38%-63%
Disease Distribution • First outbreak in the Americas (2013) • Islands in the Caribbean began reporting local cases • Previous outbreaks in: • Africa, Asia, Europe, and islands in the Indian and Pacific Oceans • Risk of outbreaks occurring in the U.S. • Vectors are present in various areas within the U.S. and its territories • Dengue and chikungunya viruses • Transmitted by the same mosquitoes • May circulate in the same area • Co-infections are possible • For an up-to-date map of countries and territories where outbreaks have occurred visit: http://www.cdc.gov/chikungunya/geo/index.html • Predicted range of chikungunya vectors by country (based on CDC, WHO, ECDC data) • States and territories with chikungunya vector populations
Clinical Findings • Incubation period: • 3 to 7 days • Acute phase: • 3 to 10 days • Main signs and symptoms: • Fever >102.5°F (39°C) • Severe pain in multiple joints • Other common signs and symptoms include: • Headache • Rash • Muscle pain • Nausea/vomiting • Conjunctivitis • Relapse of rheumatic symptoms may occur • Most common 2-3 months after initial infection • Patient is no longer viremic • Chronic chikungunya • Symptoms lasting for more than 3 months (absent viremia) • 72% to 97% of infected individuals will become symptomatic.
Case Reporting • Chikungunya infection should be considered if: • Symptoms include acute onset of fever with severe pain in multiple joints AND • The patient lives or has recently traveled to areas where chikungunya outbreaks occur • Public Health Flight should report suspected cases to: • Local/county/state/territory health departments • The Air Force (via AFDRSi) under “Any Other Unusual Condition Not Listed”
Treatment • No antiviral therapy exists. • Supportive care • Rest • Fluids • Acetominophen, paracetomol, or non-steroidal anti-inflammatory drugs (NSAIDs) may be used to reduce pain and fever • Aspirin is NOT recommended due to the possibility of bleeding in some patients • NSAIDs should NOT be used if there is a possibility the patient has dengue
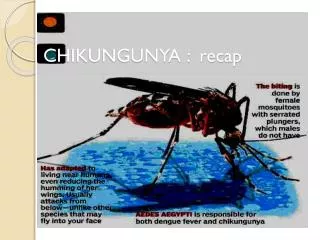
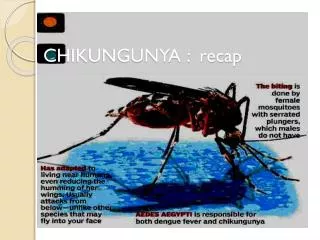
Transmission • Main mode of transmission: • Via the bite of an infected mosquito • Aedesaegypti(yellow fever mosquito) • Aedesalbopictus(Asian tiger mosquito) • Less common modes of transmission: • Mother to fetus • Via infected blood • (No evidence of transmission via breast milk) • To reduce local transmission rates: • Infected individuals should avoid mosquito contact during the first week of illness. Image courtesy of AFPMB Technical Guide No. 47
The Vectors • Aedesaegyptiand Aedesalbopictus • Small, black and white mosquitoes • Breed in containers • Aquatic cycle (from egg to adult) may be completed in as little as 7 to 9 days. • Bite during the day • Peak feeding times in the early morning and before dusk • Same mosquitoes that transmit dengue • Aedesaegypti • Guitar or lyre-shaped markings on the thorax
Prevention • No vaccine or medication can prevent chikungunya infection. • Avoid mosquito contact! • Use insect repellent such as DEET or picaridin on exposed skin. • Wear uniform or long-sleeved shirts and long pants. • Treat clothing or uniform with permethrinrepellent. • Use air conditioning. • Ensure window/door screens are tightly sealed and intact. • Reduce mosquito breeding sites • Empty or remove containers around the home or base that collect standing water.
Vector Surveillance and Reporting • Larval surveillance of containers that hold water for more than a few days. • Determines the number, type, and distribution of containers producing chikungunya vectors • USAFSAM/PHR is able to test known chikungunya vectors for the virus. • Positive mosquito pools should be reported to local/county/state/territory health departments.
Vector Control • Source reduction: • Focuses on containers that hold water and serve as larval habitats. • Helps to reduce mosquito density. • Larval control: • Larvicides (chemical and biological) applied to potential larval habitats • Adult mosquito control: • Early morning or late evening ultra-low volume (ULV) applications
For more information • CDC/Chikungunya • PAHO • CDC/PAHO Preparedness and Response for Chikungunya Virus Introduction in the Americas • Armed Forces Pest Management Board • AFPMB Dengue and Chikungunya Vector Control Pocket Guide • USAF Guide to Operational Surveillance of Medically Important Vectors and Pests • https://gumbo2.wpafb.af.mil/epi-consult/entomology Presentation Prepared by Jamie Iten