Download
1 / 15
150 likes | 282 Views
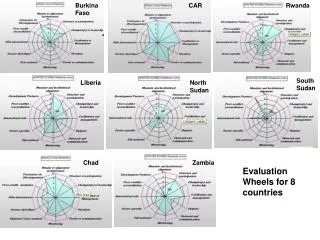
Community participation in the Burkina Faso. Dr SANOU Souleymane Managing director of health. Community participation in the Burkina Faso. 1. Introduction 2. The experiments of Community participation 3. Learnt lessons 4. Knowledge 5. Difficulties / insufficiency 6. Conclusion.

E N D
Community participation in the Burkina Faso Dr SANOU Souleymane Managing director of health
Community participation in the Burkina Faso 1. Introduction 2. The experiments of Community participation 3. Learnt lessons 4. Knowledge 5. Difficulties / insufficiency 6. Conclusion
Community participation in the Burkina Faso (1/5) Introduction • Enclosed Sahelian country • The system of health is characterized by a weak accessibility of populations in structures of health The actors of services on Community foundation: • the agents of Distribution on Community Foundation (DBC), • the Workers of Community health (ASC), • the obstetricians of village (AV) formed, • the health workers of village (ASV), • educative peers (PE), • the members of management committees (COGES), • the correspondents vaccinaux (CV),
The experiments of Community participation (2/5) 1. The Primary posts of Health (PSP) created in 1985 under Democratic and popular Revolution (operation « a village, PSP ») were the concrete expression of the organization and the participation of the village communities in the resolution of their problems of health. • PSP was kept by at least two workers of Community health (ASC) whose a village health worker (ASV) and a village obstetrician (AV). • Functions of these two categories of agents: • AV was charged
The experiments of Community participation (3/5) 2 . Initiative of Bamako • The implementation of the strategy of strengthening of the primary care of health across the Initiative of Bamako, headed with Community participation and with the levies of expenses. • The existent agents of the community become so important assistant helpers of the system of health to make participate the community in programs and in activities with which it is profitable.
The experiments of Community participation (4/5) • 3 . The laboratory of Community health of Bazèga • Offer of services on Community foundation in the field of infantile and maternal health, family planning, sensitization and social draft for the conflict against IST / HIV / AIDS, against practice of removal, taking care of diarrhoeic diseases and paludism within the village communities. • Results led the Direction of the health of the Family to adopt a Packet Minimum of Activities
The experiments of Community participation (5/5) • Surveillance on Community foundation of target diseases of the Program Elargi of Vaccination; • The surveillance of diseases with infectious potential on Community foundation (SEBAC) in the regions of the High Basins and Waterfalls
Learnt lessons (1/2) • Supplementary benefit necessary to health trainings for the access to the biggest number and to lesser expense to primary care of health • Appropriate for the improvement of the state of health of populations in the Burkina Faso • There is a difference of topics and plans of training of ASBC according to the partners who support the supervision • There is a difference in motivation and equipment of ASBC • Valuation showed that the contribution of AV in the reduction of matt mortality
Learnt lessons (2/2) • The implementation of the mechanisms of motivation of ASBC by communities was always faulty • ASBC without being skilled technicians are able of meeting needs efficiently of health of populations if they are formed well and supervised • ASBC contributes to a strong draft of communities for the implementation of the programs of health • The degree of dynamism of the agents SBC is dependent on the effectiveness of the support brought by the health workers.
Acquired (1/2) • SBC is accepted within communities • The existence of a political will to develop SBC • The growing involvement of organizations on Community foundation in the implementation of the programs of health • Technical and financial partners continue supporting certain regions in the development of SBC • The definition of a packet minimum of services in certain domains: • The existence of tools of collection of data and formulation of indicators • Exist
Acquired (2/2) • Distribution of ivermectine in the zones of risk of recrudescence of onchocercose (250 villages) • Distribution of ivermectine albendazole in the zones of transmission of the lymphatic filariose (all country) • Distribution of vitamin A to the children of less than 5 years • Distribution of contraceptive • Oral vaccination counters poliomyelitis.
Difficulties / insufficiency (1/2) • The not incorporation of the activities of ASBC in the management of the programs of health • The lack of coordination of strategies and activities of ASBC • The absence of process formalized by selection of ASBC • The not respect for the commitment of ASBC • The absence of a national strategy of the implementation of SBC • The absence of efficient and permanent strategies of motivation at the level of communities, at the level of the Ministry of Health and at other partners
Difficulties / insufficiency (2/2) • The agents SBC are under used or badly used in villages through lack of equipment, of means of displacement and failing renewal of the supplies of initial allocation • The insufficiency of training of the actors of SBC • The insufficiency of supervision, monitoring and valuation of activities SBC • The insufficiency of tale-telling of the data of activities SBC in the National System of Health Information • Insufficiency in the capitalization of experiments in subjects of SBC in communication
Conclusion • A better knowledge of Community participation must allow us to sketch a program centered on the domains of following interventions: • Health of Reproduction, • Public hygiene, • Prevention by vaccinations, • Nutrition, • Conflict counters illness • Conflict against IST and HIV / AIDS.