B-CLL
B-CLL. Morphologie: Kleine Lymphozyten mit schmalem Zyto-plasmasaum; dichtes Chromatin, z.T. zu groben Klumpen kondensiert, keine Nukleoli; Kernschatten Immunphänotyp: sIg(+), CD19/20/24 ++ , CD5 ++ , CD23 + , FMC7 -/+ , CD22 -/+ , CD10 - , HLA-DR ++ Genetik:

B-CLL
E N D
Presentation Transcript
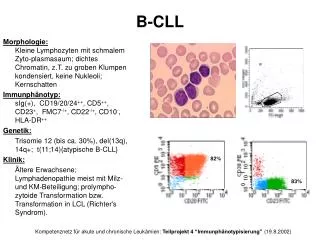
B-CLL Morphologie:Kleine Lymphozyten mit schmalem Zyto-plasmasaum; dichtes Chromatin, z.T. zu groben Klumpen kondensiert, keine Nukleoli; Kernschatten Immunphänotyp:sIg(+), CD19/20/24++, CD5++, CD23+, FMC7-/+, CD22-/+, CD10-, HLA-DR++ Genetik: Trisomie 12 (bis ca. 30%), del(13q), 14q+; t(11;14){atypische B-CLL} Klinik: Ältere Erwachsene; Lymphadenopathie meist mit Milz- und KM-Beteiligung; prolympho-zytoide Transformation bzw. Transformation in LCL (Richter's Syndrom). 82% 83% Kompetenznetz für akute und chronische Leukämien: Teilprojekt 4 “Immunphänotypisierung” (19.8.2002)
B - PLL Morphologie: > 55% der Zellen mit verklumptem Chromatin und prominentem vesikulärem Nukleolus, deutlicher Zyto-plasmasaum Immunphänotyp: sIg++, CD19/20/24++, FMC7++, CD22++, CD5+/-, CD23-/+, CD10-, HLA-DR++ Genetik: 14q+(14q32) Klinik: Alter (Median): 70 Jahre; Hyperleukozytose (Prolymphozyten > 55%), Splenomegalie, keine Lymphadenopathie, KM-Infiltration diffus oder interstitiell-nodulär; meist aggressiver Verlauf 91% 9% 95% Kompetenznetz für akute und chronische Leukämien: Teilprojekt 4 “Immunphänotypisierung” (19.8.2002)
T - PLL Morphologie: mittelgroße Zellen mit deutlichem Zy-toplasmasaum, mäßig kondensiertes Chromatin, prominenter Nukleolus; "small-cell variant" Immunphänotyp: CD2+, CD3+, CD5+, CD7+, CD4+ (65%), CD4+8+ (21%), CD4-8+ (selten), TZR+, CD25-, CD38+/-, TdT- Genetik: inv 14 (q11 q32), Trisomie 8q Klinik: 1% aller CLL, aber 20% aller PLL, Hyperleukozytose, häufig Haut- und Schleimhautinfiltrate, aggressiver Verlauf Kompetenznetz für akute und chronische Leukämien: Teilprojekt 4 “Immunphänotypisierung” (19.8.2002)
Mantelzell-Lymphom (cc-NHL) Morphologie: Kleine bis mittelgroße Lymphoidzellen, irreguläre Kerne, z.T. eingekerbt, vereinzelt mit großen Nukleoli; lymphoblastoide Variante Immunphänotyp: sIg++, CD5+, CD10-, CD23-, CD11c-, HLA-DR++, CD43+ Genetik: t(11;14)(q13;q32); Onkogen: PRAD1/CCND1 Cyclin D1 Klinik: Ältere Erwachsene, M > F, meist generalisiertes Stadium bei Diagnose (auch extranodale Manif., z.B. GIT), medianes Überleben 3-5 Jahre 83% 20% Kompetenznetz für akute und chronische Leukämien: Teilprojekt 4 “Immunphänotypisierung” (19.8.2002)
Follikuläres NHL (leukämisch) • Morphologie: • Heterogene Zellpopulation aus Centrocyten und Centroblasten • Immunphänotyp: • sIg++, CD5-, CD10+/-, CD23-/+, CD11c-, HLA-DR++ • Genetik: • t(14;18)(q32;q21) mit Rearrangement des bcl-2 Gens • Klinik: • Erwachsene, F : M = 1 : 1, ca. 40% aller NHL bei Erwachsenen; meist Splenomegalie und Lymphadenopathie, leukämischer Verlauf bei ca. 4.5 - 23% der Fälle. 98% 67% 99% Kompetenznetz für akute und chronische Leukämien: Teilprojekt 4 “Immunphänotypisierung” (19.8.2002)