Download
1 / 34
340 likes | 513 Views
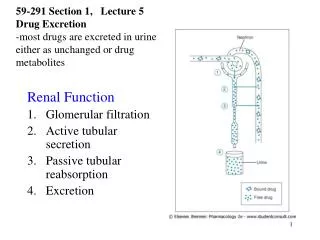
Glomerular and tubular dysfunctions. Tatár M. Basic kidney functions. Water and electrolyte homeostasis Acid – base balance Elimination of waste products and ingested chemicals Hormone production. Mechanisms of renal excretion. 180 l glomerular filtrate per day (2 ml/s)

E N D
Glomerular and tubular dysfunctions Tatár M.
Basic kidney functions • Water and electrolyte homeostasis • Acid – base balance • Elimination of waste products and ingested chemicals • Hormone production
Mechanisms of renal excretion • 180 l glomerular filtrate per day (2 ml/s) • 99% - back reabsoption • Renal perfusion at rest = 20% of cardiac output (this is higher than in heart, brain and liver
Glomerular filtration rate • Balance of hydrostatic and osmotic pressures acting across diffusion barrier (endotelium fenestrae, basement nenbrane, slit diaphragms betweens the podocytes) • Factors determining GFR: • Surface area (1 milion nephrons within each kidney) • Permeability • Net filtration pressure (NFP) across diffusion barrier
Factors determining GFR • surface area • permeability filtration koefficient (Kf) GFR =Kf x NFP NFP = PGC – PT – GC 24 = 60 - 15 - 21 mmHg
Disturbances of glomerular function (1) • Decrease of glomerular filtration • renal blood flow stenosis of renal artery • glomerular capillary hydrostatic pressure (PGC) hypovolemia, circulatory shock • hydrostatic pressure in Bowman´s capsule (PT) block of fluid flow ( intra- and extrarenal) • concentration of plasma proteins (GC) • Kf effective filtration surface area
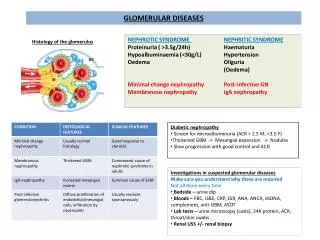
Disturbances of glomerular function (2) B. Increase of glomerular permeability Proteinuria • Glomerular proteinuria • Size-selective properties of the glomerulus • Charge-selective propeties of the glomerulus • Hamodynamic forces operating across the glomerulus
Glomerular proteinuria • Selective proteinuria • Albumin • Small amount of low-molecular globulins • Non-selective proteinuria • Albumin • Globulins of various molecular weight
Tubular proteinuria • excretion of low molecular proteins • 1-microglobulin, 2-microglobulin
Overload (prerenal) proteinuria • Small molecular weight proteins can rise when are synthetised in excess • Tissue degradedproducts • Proteins of acute phase (pyretic proteinuria) • Myoglobin (rhabdomyolysis) • Ligfht immunoglobulin chains (myeloma)
Proteinuria • Healthy adult subject • No more than 150 mg/day • Small proteinuria • 1 g/day • Haevy proteinuria • 3,5 g/day and more • Nephrotic syndrome (10 – 30 g/day)
Renal hematuria • Glomerular • Abnormally increased permeability • Non-glomerular • Rupture of tumor or cyst vessels • Bleading from urinary tract
Relation between the reduction of GFR and excretion function of kidneys GF retention of substrates 1. urea, creatinín 2. phosphates, K+, H+ 3. NaCl
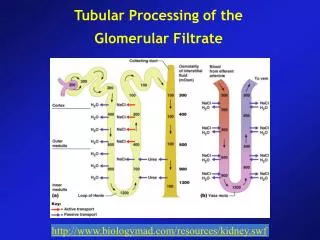
Reabsorption of glucose, amino acids, Na, K, Cl, H2O Proximal tubule Thick ascending limb of loop of Henle Distale tubule
Disturbances of tubular functions Transport maximum • Tubular proteinuria • Glucosuria • Aminoaciduria • Diabetes insipidus • Neurogenic ( ADH) • Nephrogenic (insensitivity of the renal tubule to ADH) • Osmotic diuresis • Pressure of large quantities of unreabsorbed solutes in the renal tubules increase in urine volume • Unreabsorbed solutes in the proximal tubules „hold water in the next tubules“
Hydrogen ion secretion and bicarbonate reabsorption Renal tubular acidosis - impairment of the ability to make the urine acidic - chronic renal disease – reduction of secreted hydrogen ion because of impaired renal tubular production of NH4+
Loop of Henle and production of concentrated urine - Permeability for water and NaCl - ADH
Disturbances of kidney ability to concentrate urine • Disturbances of water reabsorption - diabetes insipidus • Disturbances of the production of medullar hyperosmolarity - osmotic diuresis - blood flow in vasa recta - morphologic deformations of medulla
Nephrotic syndrome • Proteinuria: 3.5 g or more of protein in the urine per day • Minimal changes of glomerular membrane: 90% albumin (selective proteinuria) • Hypoproteinemia (hypoalbuminemia) • Mechanisms: proteinuria + • Protein loss by stool • Plasma proteins are shifted to extravascular space • Increased albumin katabolism • Inadequately increase albumin synthesis in liver • Hyperlipidemia • Incresed lipoprotein synthesis in liver • Generalised edema
Mechanisms of edema in nephrotic syndrome (NS) • Classis theory • Hypoalbuminemia plasma oncotic pressure hypovolemia R-A-A + ADH Na + water retention • !!! But hypovolemia is present only in 30% of patients suffering from NS; plasma renin activity and aldosteron are decreased • Two groups of patients with NS: • Hypovolemia and R-A-A activity - small glomerular abnormalities • Hypervolemia without R-A-A activation - more serious morphological abnormalities
Pathophysiology of edema formation • Extracellular fluid volume is determined by the balance between Na intake and its renal excretion • Common feature: renal salt retention despite progressive expaansion of ECF volume • Primary abnormality of the kidney • Secondary response to some disturbances in the circulation
Primary edema (overfill) • Primary defect in renal sodium excretion • Hyperevolemia leads to high cardiac output • R-A-A, ADH, sympathetic activity Examples: blomerulonephritis, renal failure
Secondary edema (underfill) • Response of normal kidnay to actual or sensed underfilling of the circulation • Primary disturbances within the circulation secondary triggers renal sodium retention • R-A-A, ADH, sympathetic activity • Effective arterial blood volume