Download

1 / 17
0 likes | 10 Views
A study on patients with resolved atrial fibrillation reveals they still face higher risks of stroke or TIA compared to those without atrial fibrillation. The research, based on UK primary care records, emphasizes the ongoing need for anticoagulant treatment in such patients to mitigate risks, even when recurrent atrial fibrillation is not clearly documented.

E N D
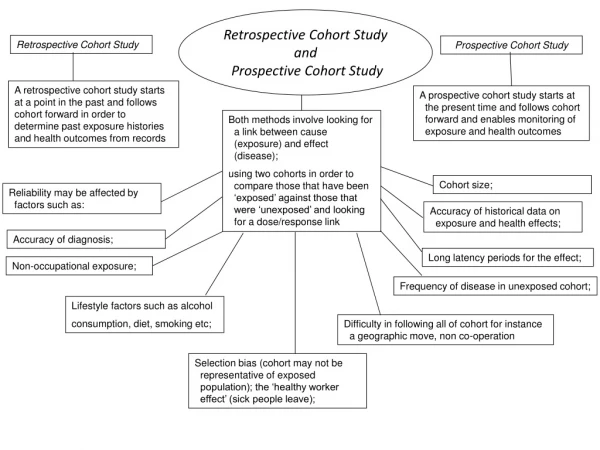
Risk of stroke and transient Risk of stroke and transient ischaemic a diagnosis of resolved atrial fibrillation: a diagnosis of resolved atrial fibrillation: retrospective cohort retrospective cohortstudies. ischaemicattack in patients with attack in patients with studies. Nicola J Adderley, KrishnarajahNirantharakumar, Tom Marshall. BMJ 2018 PRESENTER: WEN-CHING LAN DATE: 2018/10/17
Introduction Introduction •Atrial fibrillation is the most common sustained cardiac arrhythmia and is associated with a fivefold increase in risk of stroke. •Treatment with anticoagulants reduces the risk by about two thirds. •Patients in whom atrial fibrillation is considered resolved might in fact have paroxysmal or persistent subtypes, or atrial fibrillation that might recur. 1
Objectives Objectives To determine rates of stroke or transient ischaemic attack (TIA) and all cause mortality in patients with a diagnosis of “resolved” atrial fibrillation compared to patients with unresolved atrial fibrillation and without atrial fibrillation. 2
Methods Methods Data source •We extracted datasets from The Health Improvement Network (THIN), a database of electronic primary care records from UK general practices using Vision software. •THIN comprises coded data on patient characteristics, diagnoses, prescriptions, consultations, and investigations. 3
Methods Methods Study design •Adults aged 18 years or more and registered for at least 365 days before the census date were eligible for inclusion. •stroke or TIA (primary outcome) and all cause mortality (secondary outcome) •The study period was 1 January 2000 to 15 May 2016. •The exposure was a clinical code of “atrial fibrillation resolved. •The index date was the coding date for resolved atrial fibrillation plus 180 days. •End date(patient left dataset or transferred out, death, study end date) or event date. 4
Methods Methods Analysis •Frequency of resolved atrial fibrillation 1. χ2 test to calculate P values for trends over time. •Incidence of stroke or TIA and mortality 1. χ2 / t tests 2. Poisson regression 3. sensitivity analysis 4. The Nelson-Aalen cumulative hazard function 5. subgroup analysis 5
Methods Methods Definitions of variables •clinical code→ AF, paroxysmal AF, resolved AF, stroke, TIA(ischaemic stroke, haemorrhagic stroke) Heart failure, ischaemic heart disease, diabetes, hypertension •THIN demography file→ BMI, Smoking status, Alcohol consumption, ethnicity (×1.210 if black) •eGFR=186×(creatinine/88.4)-1.154×age-0.203×(0.742 if female) •Charlson comorbidity index score •CHA2DS2-VASc scores •Current statin or anticoagulant (warfarin, parenteral anticoagulants, other vitamin K antagonists, and novel oral anticoagulants. )→ 90 days before the index date 6
Methods Methods Missing data •Variables were complete except for Townsend score, smoking status, drinking status, BMI, and eGFR. •this assumed missingness was not associated with the outcome. •We carried out a sensitivity analysis using multiple imputation (10 imputations, chained equations) to replace missing data; this made no difference to the results. 7
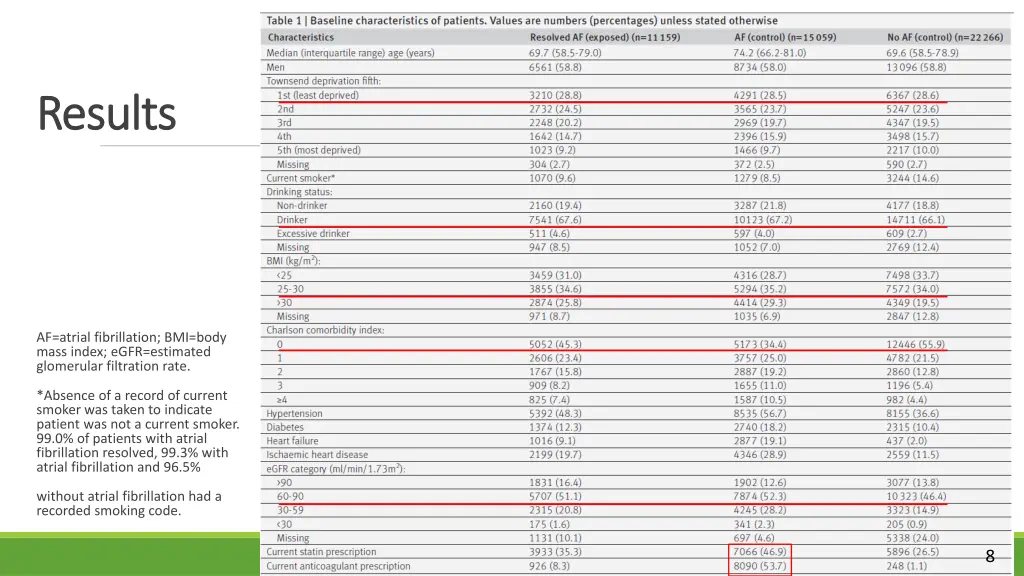
Results Results AF=atrial fibrillation; BMI=body mass index; eGFR=estimated glomerular filtration rate. *Absence of a record of current smoker was taken to indicate patient was not a current smoker. 99.0% of patients with atrial fibrillation resolved, 99.3% with atrial fibrillation and 96.5% without atrial fibrillation had a recorded smoking code. 8
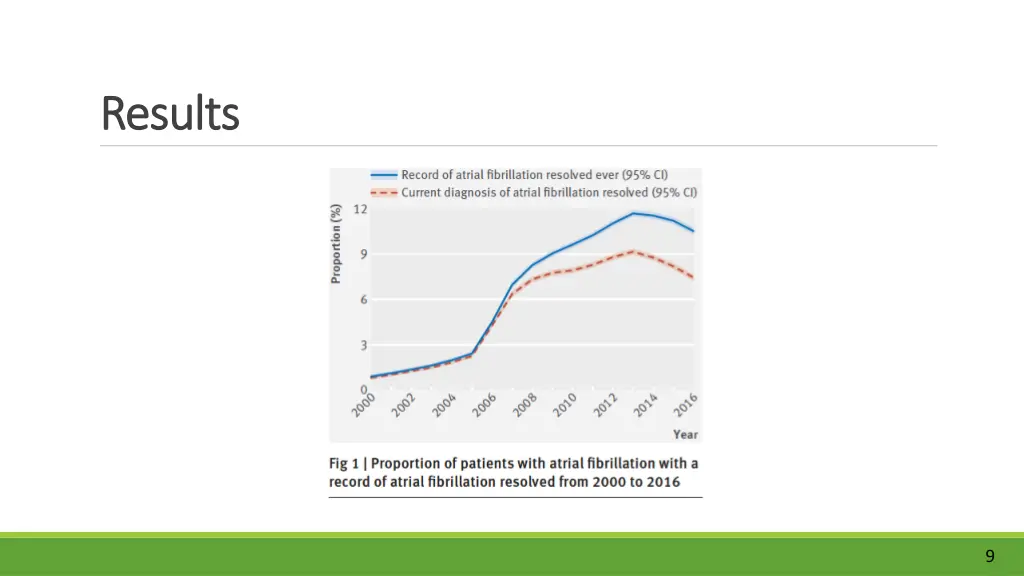
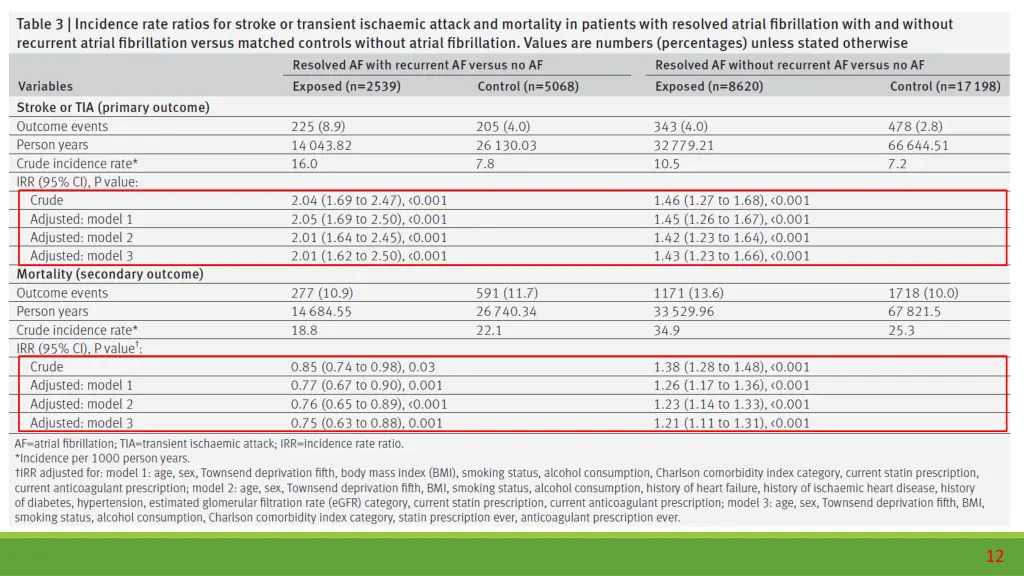
Results Results 9
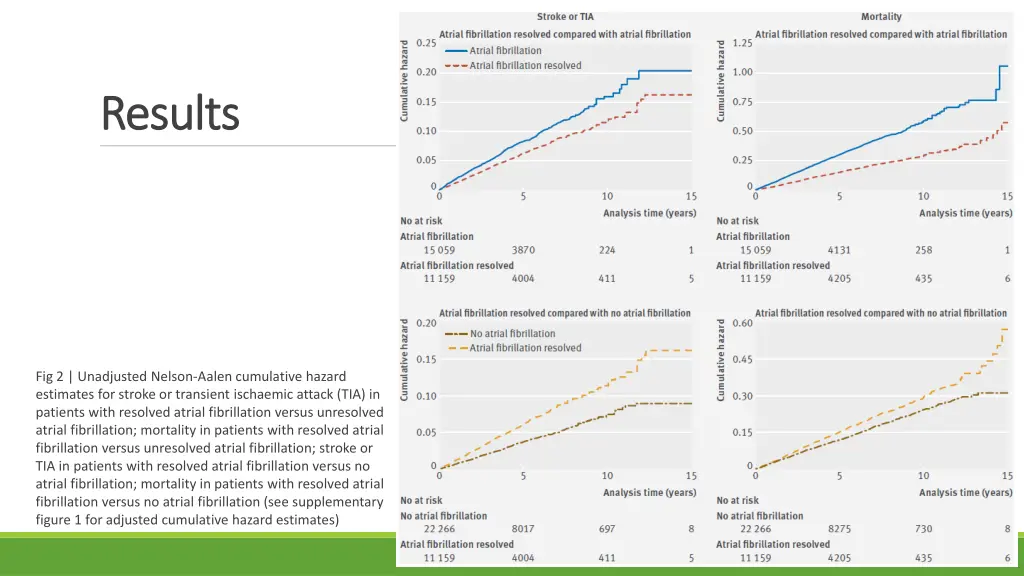
Results Results Fig 2 | Unadjusted Nelson-Aalen cumulative hazard estimates for stroke or transient ischaemic attack (TIA) in patients with resolved atrial fibrillation versus unresolved atrial fibrillation; mortality in patients with resolved atrial fibrillation versus unresolved atrial fibrillation; stroke or TIA in patients with resolved atrial fibrillation versus no atrial fibrillation; mortality in patients with resolved atrial fibrillation versus no atrial fibrillation (see supplementary figure 1 for adjusted cumulative hazard estimates)
Strengths Strengths / limitations / limitations Strengths 1. large general practice database that is generalisable to the UK population and comprises routine clinical data used in decision making by general practitioners. Limitations 1. Coded recording, Ethnicity, Townsend scores of may not accurately 2. Some patients receiving anticoagulants might not have been identified if the treatment was managed entirely in secondary care, 3. death is a competing risk. 13
Conclusion Conclusion •Patients with resolved atrial fibrillation remain at higher risk of stroke or TIA than patients without atrial fibrillation. •The risk is increased even in those in whom recurrent atrial fibrillation is not documented. •Guidelines should be updated to advocate continued use of anticoagulants in patients with resolved atrial fibrillation. 14
Thanks for listening. Thanks for listening.
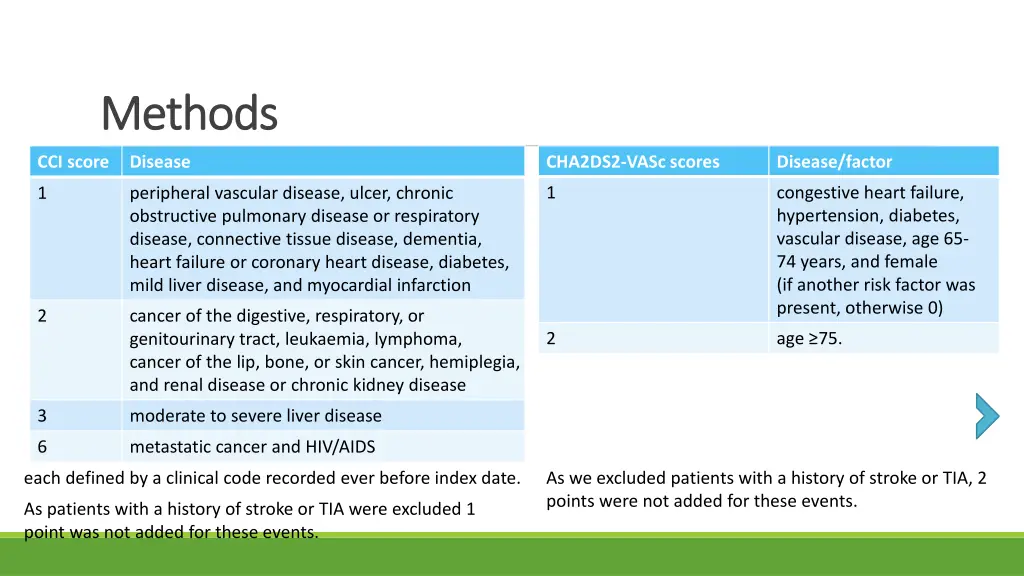
Methods Methods CCI score Disease CHA2DS2-VASc scores Disease/factor 1 congestive heart failure, hypertension, diabetes, vascular disease, age 65- 74 years, and female (if another risk factor was present, otherwise 0) 1 peripheral vascular disease, ulcer, chronic obstructive pulmonary disease or respiratory disease, connective tissue disease, dementia, heart failure or coronary heart disease, diabetes, mild liver disease, and myocardial infarction 2 cancer of the digestive, respiratory, or genitourinary tract, leukaemia, lymphoma, cancer of the lip, bone, or skin cancer, hemiplegia, and renal disease or chronic kidney disease 2 age ≥75. 3 moderate to severe liver disease 6 metastatic cancer and HIV/AIDS each defined by a clinical code recorded ever before index date. As we excluded patients with a history of stroke or TIA, 2 points were not added for these events. As patients with a history of stroke or TIA were excluded 1 point was not added for these events.