Download
1 / 1
30 likes | 272 Views
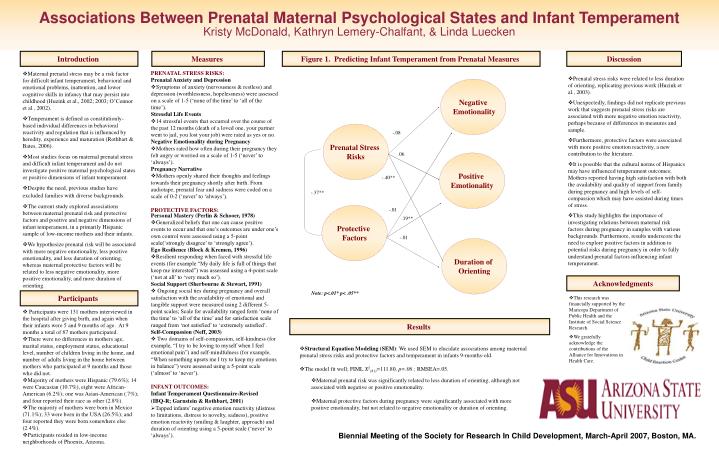
Associations Between Prenatal Maternal Psychological States and Infant Temperament Kristy McDonald, Kathryn Lemery-Chalfant, & Linda Luecken. Introduction. Measures. Figure 1. Predicting Infant Temperament from Prenatal Measures. Discussion. PRENATAL STRESS RISKS:

E N D
Associations Between Prenatal Maternal Psychological States and Infant TemperamentKristy McDonald, Kathryn Lemery-Chalfant, & Linda Luecken Introduction Measures Figure 1. Predicting Infant Temperament from Prenatal Measures Discussion PRENATAL STRESS RISKS: Prenatal Anxiety and Depression • Symptoms of anxiety (nervousness & restless) and depression (worthlessness, hopelessness) were assessed on a scale of 1-5 (‘none of the time’ to ‘all of the time’). Stressful Life Events • 14 stressful events that occurred over the course of the past 12 months (death of a loved one, your partner went to jail, you lost your job) were rated as yes or no. Negative Emotionality during Pregnancy • Mothers rated how often during their pregnancy they felt angry or worried on a scale of 1-5 (‘never’ to ‘always’). Pregnancy Narrative • Mothers openly shared their thoughts and feelings towards their pregnancy shortly after birth. From audiotape, prenatal fear and sadness were coded on a scale of 0-2 (‘never’ to ‘always’). PROTECTIVE FACTORS: • Personal Mastery (Perlin & Schooer, 1978) • Generalized beliefs that one can cause positive events to occur and that one’s outcomes are under one’s own control were assessed using a 5-point scale(‘strongly disagree’ to ‘strongly agree’). Ego Resilience (Block & Kremen, 1996) • Resilient responding when faced with stressful life events (for example “My daily life is full of things that keep me interested”) was assessed using a 4-point scale (‘not at all’ to ‘very much so’). Social Support (Sherbourne & Stewart, 1991) • Ongoing social ties during pregnancy and overall satisfaction with the availability of emotional and tangible support were measured using 2 different 5-point scales; Scale for availability ranged form ‘none of the time’ to ‘all of the time’ and for satisfaction scale ranged from ‘not satisfied’ to ‘extremely satisfied’. Self-Compassion (Neff, 2003) • Two domains of self-compassion, self-kindness (for example, “I try to be loving to myself when I feel emotional pain”) and self-mindfulness (for example, “When something upsets me I try to keep my emotions in balance”) were assessed using a 5-point scale (‘almost’ to ‘never’). INFANT OUTCOMES: Infant Temperament Questionnaire-Revised • (IBQ-R; Garnstein & Rothbart, 2001) • Tapped infants’ negative emotion reactivity (distress to limitations, distress to novelty, sadness), positive emotion reactivity (smiling & laughter, approach) and duration of orienting using a 5-point scale (‘never’ to ‘always’). • Maternal prenatal stress may be a risk factor for difficult infant temperament, behavioral and emotional problems, inattention, and lower cognitive skills in infancy that may persist into childhood (Huzink et al., 2002; 2003; O’Connor et al., 2002). • Temperament is defined as constitutionly-based individual differences in behavioral reactivity and regulation that is influenced by heredity, experience and maturation (Rothbart & Bates, 2006). • Most studies focus on maternal prenatal stress and difficult infant temperament and do not investigate positive maternal psychological states or positive dimensions of infant temperament. • Despite the need, previous studies have excluded families with diversebackgrounds. • The current study explored associations between maternal prenatal risk and protective factors and positive and negative dimensions of infant temperament, in a primarily Hispanic sample of low-income mothers and their infants. • We hypothesize prenatal risk will be associated with more negative emotionality, less positive emotionality, and less duration of orienting, whereas maternal protective factors will be related to less negative emotionality, more positive emotionality, and more duration of orienting. • Prenatal stress risks were related to less duration of orienting, replicating previous work (Huzink et al., 2003). • Unexpectedly, findings did not replicate previous work that suggests prenatal stress risks are associated with more negative emotion reactivity, perhaps because of differences in measures and sample. • Furthermore, protective factors were associated with more positive emotion reactivity, a new contribution to the literature. • It is possible that the cultural norms of Hispanics may have influenced temperament outcomes; Mothers reported having high satisfaction with both the availability and quality of support from family during pregnancy and high levels of self-compassion which may have assisted during times of stress. • This study highlights the importance of investigating relations between maternal risk factors during pregnancy in samples with various backgrounds. Furthermore, results underscore the need to explore positive factors in addition to potential risks during pregnancy in order to fully understand prenatal factors influencing infant temperament. Negative Emotionality Prenatal Stress Risks -.08 .06 Positive Emotionality -.40** -.37** Protective Factors -.01 .19** -.01 Duration of Orienting Acknowledgments Note: p<.01* p< .05** Participants • This research was financially supported by the Maricopa Department of Public Health and the Institute of Social Science Research. • We gratefully acknowledge the contributions of the Alliance for Innovations in Health Care. • Participants were 131 mothers interviewed in the hospital after giving birth, and again when their infants were 5 and 9 months of age. At 9 months a total of 87 mothers participated. • There were no differences in mothers age, marital status, employment status, educational level, number of children living in the home, and number of adults living in the home between mothers who participated at 9 months and those who did not. • Majority of mothers were Hispanic (79.6%); 14 were Caucasian (10.7%), eight were African-American (6.2%); one was Asian-American (.7%); and four reported their race as other (2.8%). • The majority of mothers were born in Mexico (71.1%); 33 were born in the USA (26.5%); and four reported they were born somewhere else (2.4%). • Participants resided in low-income neighborhoods of Phoenix, Arizona. Results • Structural Equation Modeling (SEM): We used SEM to elucidate associations among maternal prenatal stress risks and protective factors and temperament in infants 9-months-old. • The model fit well; FIML X2(81)=111.80, p=.06 ; RMSEA=.05. • Maternal prenatal risk was significantly related to less duration of orienting, although not associated with negative or positive emotionality. • Maternal protective factors during pregnancy were significantly associated with more positive emotionality, but not related to negative emotionality or duration of orienting. Biennial Meeting of the Society for Research In Child Development, March-April 2007, Boston, MA.