Download
1 / 59
590 likes | 823 Views
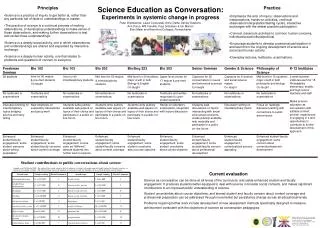
Evaluation of Current Operational Stress Management in the UK Military. Or….. the Seductions of Screening and the Disappointments of Debriefing. Major N Jones Academic Centre for Defence Mental Helath. What are we trying to achieve?. We want to….

E N D
Evaluation of Current Operational Stress Management in the UK Military Or….. the Seductions of Screening and the Disappointments of Debriefing Major N Jones Academic Centre for Defence Mental Helath
We want to…. • Promote resilience, courage, independence, toughness etc…………. • But at the same time encourage those with mental health problems to present when they need to
We don’t want to…. • Before deployment: increase anxiety, increase risk avoidance and reduce confidence • During: reduce resilience, courage etc….. • After deployment : increase helplessness, vulnerability and mental distress ; decrease resilience, coping and self efficacy ; swamp services with non mental health problems; label people inappropriately • Long time after: cause mistrust, rumour and conspiracy; add to the Pensions bill
Primary mental health outcomes (Regulars only) ► Hotopf et al. Lancet 2006: 367: 1731-1741
Primary mental health outcomes (Regulars only) Hotopf et al. Lancet 2006: 367: 1731-1741
Non-military risk factors for PTSD: (Op Telic) Some are more vulnerable than others………………. • Being younger • Lower education • Being single • Rank • Childhood adversity Iversen et al, Psych med 2008
Military risk factors for PTSD: (UK Op Telic) In theatre, some are more vulnerable than others………………. • Being deployed for <13 months in last 3 years • Not receiving a homecoming brief • Work in theatre did not match trade or experience • Being in the Reserves • Time spent in a forward area • Thought that they might be killed • Low morale
What could you do to prevent psychological injury? • Training • Pre deployment screening • Pre deployment psycho-education • Post deployment psycho-education • Decompression • Peer group support (“TRIM”) • Battlemind
What could you do to prevent psychological injury? • Pre deployment screening? • Pre deployment psycho-education • Post deployment psycho-education • Decompression • Peer group support (“TRIM”) • Battlemind
The seductions of screening! • Save people and families from psychiatric disorder • Save commanders from ineffective personnel • Save the Chancellor from paying war pensions
UK Screening Study Op Telic Main Study, 2005 n=1885 (69%) Screening study (completed 2002) n=2800 Controls Rona et al, BMJ 2006
Test characteristics: (n=1885) Caseness at baseline as a predictor of caseness at follow-up Rona et al, BMJ 2006
Barriers to mental health screening: qualitative study • Most people would not answer mental health questionnaires honestly to Defence Medical Services • “system leaks” • “effects on career” • “stigma” • Minority were seeking mental health care outside Defence Medical Services French, Jones, Wessely, Rona, JMS 2004
What could we do to prevent psychological injury? • Training • Screening • Pre deployment psycho-education (briefing)? • Post deployment psycho education? • Decompression • Post deployment psychological debriefing • Peer group support (“TRIM”) • Battlemind
Pre-Operational Stress Briefing: does it have any effect? 279 + - 456 • TELIC 1 RN & RM regular personnel who are in King’s health and wellbeing study • No significant differences in common mental health disorders, PTSD or alcohol misuse • No differences for experiencing problems during or post-deployment or for marital satisfaction • No evidence that a pre-deployment stress briefing reduced psychological distress • The brief appeared to do no harm. Sharpley et al Occ med 008)
The Sheffield trials of psycho education ‘High risk’ of PTSD - screened positive for acute stress disorder (ASD). No evidence that giving self help leaflets helped Ratings of the usefulness of the self-help booklet were very high in all groups 116 ASD pts received self-help booklet 111 ASD pts did not 120 controls with no ASD did not receive a booklet PTSD, anxiety and depression all reduced in all groups, BUT…………. No between group differences in psychological symptoms or on ratings of quality of life Scholes et al Beh Res & Therapy 2007
.15 .1 .05 0 20 30 40 50 60 age p1, taughtst2 == 0 p1, taughtst2 == 1 p1, taughtst2 == 2 It’s not what you do but the way that you do it….. Stress Education and PCL score Remembers as not useful Does not remember having a brief Remembers as useful Langston, Greenberg, Iversen, Fear, Wessely – Occ Med 2008
Prevention - Conclusion Part 1 The best prevention before deployment is preparation for combat – morale, leadership, tough realistic training*, military skills etc…..there is little evidence that mental health services have much to do with it! *‘Well Warrior effect’
What could you do to prevent psychological injury? • Pre deployment screening • Pre deployment psycho-education? • Post deployment psycho education • Decompression? • Post deployment psychological debriefing • Peer group support (“TRIM”) • Battlemind
Decompression Can we assist recovery from Ops?
Decompression Process Overview • Those who fight together should unwind together • Part of Post Operational Stress Management • Often referred to as Third Location Decompression • Currently for UK AF, takes place in Cyprus • Now for all Iraq and Afghanistan formed units • 796 personnel surveyed in 1st Wave • 2nd wave of 6000 currently being analysed
Process and Activities • Cyprus • Mental Health Brief • Coming Home Brief • Social Event • Beach Activities • Entertainment Show • Access to Mental Health Personnel • Booze!!
Do you think that the decompression briefings will make going home easier for you?
Do you think decompression has been helpful in letting you know how to deal with unpleasant incidents that occur during a tour?
I would not seek help for a mental health problem because…………
Have you had a deployment experience that was so frightening, horrible, or upsetting that DURING THE PAST MONTH you had…..
Traumatic Distress Symptoms • 124 (16%) of respondents endorsed 2 or more symptoms on the 4 Item PTS Scale. These are broken down as follows: • 4 Symptoms 21 (3%) • 3 Symptoms 40 (5%) • 2 Symptoms 63 (8%)
What is the natural history of PTSD? PTSD ‘caseness’ of patients directly involved in a raid over time. Data from Richards (1997) The Prevention of PTSD after armed robbery: the impact of a training programme within Leeds Permanent Building Society.
Prevention – Conclusion Part 2 • Subjectively positive- Decompression generally helpful • Stigma affects about a third of people • About 1/6th have significant trauma Sxs very early on • How do we signpost effectively to helping services and overcome stigma?
Post Deployment Interventions for Operational Stress Injuries
Post deployment briefings – useful? Military risk factors for psychological illness: • Thought might be killed • Morale • Time spent in forward area • Being in the Reserves • *Not receiving a homecoming brief • Work in theatre did not match trade or experience • Being deployed for <13 months in last 3 years *Adjusted odds ratio 1.84 with 95% CI of 1.3-2.62 Iversen AC Psychol Med. 2008
What could we do to prevent psychological injury? • Pre deployment screening • Pre deployment psycho-education? • Post deployment psycho education • Decompression? • Post deployment psychological debriefing • Peer group support (“TRIM”) • Battlemind
Royal Navy TRiM Study Outcomes
What is TRiM? (Traumatic Risk Management) • Essentially a peer support programme: • General support • Formal strategic planning as soon as possible after the incident • Identifying all those at risk using a structured template • Organising no intervention, individual and small group risk assessment • Briefing (psycho education) to larger groups • Risk assessments using a 10 item risk scale at an early stage, at 28 days and at a later time if early problems persist • The strategy is embedded in continuous mentoring, general support and advice about self-management • Referral when and if required.
Combat troops • Medical personnel • Those exposed to indirect fire • Quick Reaction Forces • Rescuers and helpers • PRE INCIDENT STRATEGIES • Risk Management Policy • Ongoing practitioner training • Pool of practitioners OPERATIONAL or COMBAT EVENT • POST INCIDENT SUPPORT • Effective Site Management Strategies • Planning the Strategy (Planning Meeting) • Individual TRiM Assessments • Small Group TRiM Assessments • Briefing Meeting and Information Leaflets • FIRST LINE SUPPORT • Monitor Closely • Use Internal Support Systems • Remove from Source of Stress if Possible First TRiM Assessment Liaison Second TRiM Assessment • SECOND LINE SUPPORT • Medical Officer • Padre • Welfare Personnel • TRiM team leader Problem Resolves Problem Continues Mental Health Service Referral Problem Continues Target Groups Likely to be Exposed to Traumatic Events TRiM Overview 40 Early Internal Referral
6 TRiM Trained 6 Non-TRiM Trained 18 months Follow-up 18 months Follow-up Between Groups Comparison TRiM Study 12 Ships Randomised to 2 conditions
Harm & Stigma • Over a 12 to 18 month period, no evidence that TRiM does any harm. • No evidence to suggest that it has altered stigmatising beliefs. • Non-specific indications that of beneficial organisational outcomes (reduced disciplinary breaches) and benefits to mental health. (TRiM trained ships maintained mental health, non-trained got worse).
Exposure to Trauma • Few traumatic incidents and therefore TRiM was not used “in anger” very often. • Very difficult to say anything about the risk assessment element (the key ingredient).
Acceptability • Those in contact with TRiM in practice generally found it acceptable and rated it more highly than other forms of in-service support after traumatic incidents. • Junior ranks, (those at risk of developing mental health problems), were sceptical that their peer group could offer emotional support, less of an issue for Seniors and Officers.
Signposting • Most personnel had never heard of military mental health services!!! (a potential substantial barrier to accessing care!)
Quality of Stress Briefs • Only half of the sample remembered being briefed in anyway about stress. • Those attending poor mental health briefings were more distressed than those receiving good briefings and those who had never been briefed at all. • More effort is required in terms of training and quality assurance in relation to psycho-education within the Services.
Alcohol • Alcohol remains a significant issue in those surveyed; high numbers of Navy personnel were drinking to excess and binge drinking. Their alcohol misuse was worse than age matched civilian samples.
Corporate Approach to Stress • The sample reported that the Navy had improved in its approach to stress by using TRiM. • Most personnel, regardless of rank, would act appropriately if they were confronted with a distressed individual and would act to prevent harm and ensure safety. • TRiM should become an option for the chain of command to utilise in support of their personnel but at present should not become SOP.
Requirement for TRiM • Within lower threat environments, such as the ships studied here, it seems unlikely that, from current evidence, the provision of TRiM could be regarded as an essential ingredient in the Royal Navy duty of care. • TRiM may have positive effects on attitudinal change and morale in years to come and also that it is more likely to be of utility within high threat environments*. • *Currently under investigation
TRiM and Educational Strategies in PTSD Does TRiM improve practitioner/comander attitudes and behaviour? • Examined the effect TRiM upon stigmatising beliefs, attitudes to stress and mental illness. • Training significantly improved attitudes about PTSD, stress, and help-seeking in TRiM trained personnel. • TRiM trained personnel were more likely to have a positive view of help-seeking for a mental health problem from TRiM trained personnel but were more likely to have a negative view of seeking help from command. • TRiM could be a promising anti-stigma program within organizational settings and appears to do no harm. Gould et al 2007