Download
1 / 32
360 likes | 723 Views
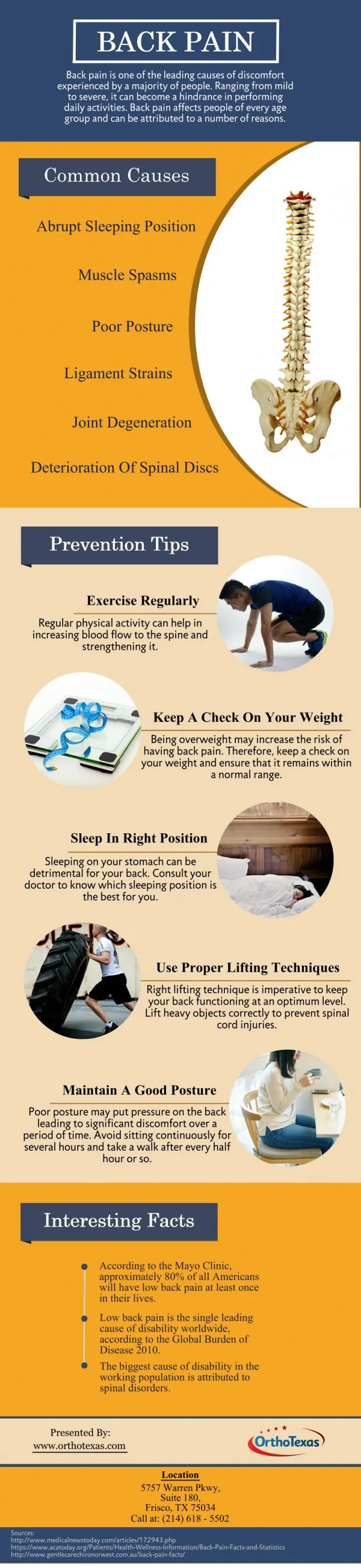
Back Pain. Examination, assessment, red flags, Good Back Guide. Jon Dixon, Bradford VTS. Causes of back pain 1. Mechanical - Muscles and ligaments Local tenderness, muscle spasm, loss of lumbar lordosis, percussion tenderness over spinous process NO MOTOR/SENSORY/REFLEXIC LOSS.

E N D
Back Pain Examination, assessment, red flags, Good Back Guide. Jon Dixon, Bradford VTS
Causes of back pain 1 Mechanical - Muscles and ligaments Local tenderness, muscle spasm, loss of lumbar lordosis, percussion tenderness over spinous process NO MOTOR/SENSORY/REFLEXIC LOSS
Causes of low back pain 2 • Radicular low back pain • Herniated intervertebral disc commonest cause but can be foraminal stenosis sec. OA / tumours / infection (rare) • TOP TIP not all pain referred down leg is sciatica (facet joint disease / hip / SIJ / piriformis syndrome etc.)
Piriformis syndrome Pain from piriformis muscle – irritation of sciatic nerve passing deep or through it Pain on resisted abduction / external rotation of leg
Causes of low back pain 3 • Lumbar Spinal Stenosis • Subtle presentation. • Bilateral radicular signs should alert to possibility. • Pain on walking- worse on flat –(eases if hunched over – shopping trolley sign!) • Can be mistaken for Claudication. • Admit if progressive / or else CT scan.
Causes of low back pain 4 • Inflammatory – Ankylosing Spondylitis • Difficult to diagnose if early stages but: • Morning stiffness for > 30 minutes • Pain that alternates from side to side of lumbar spine • Sternocostal pain • Reduced chest expansion • Schobers test
Red Flags • Weight loss, fever, night sweats • History of malignancy • Acute onset in the elderly • Neurological disturbance Bilateral or alternating symptoms • Sphincter disturbance • Immunosuppression • Infection (current/recent) • Claudication or signs of peripheral ischaemia • Nocturnal pain
Yellow Flags 2 Factors prolonging back pain • Internal factors-Opioid dependency • “External controller” patient-type; learned helplessness; factitious disorder • Mental health- depression or anxiety • Interpersonal factors "Sick role“ • Stressors in relationships • Environmental / societal factors- Disability payments / Litigation / Malingering
Structural MechanicalFacet joint arthritisProplapsed intervertebral discSpondylolysis / Spinal stenosis Inflammatory SacroiliitisSpondyloarthropathies Infection Metabolic Osteoporotic vertebral collapsePaget's diseaseOsteomalacia Neoplasm Ca Prostate Ca Breast Causes of back pain
Referred pain • Pleuritic pain • Upper UTI / renal calculus • Abdominal aortic aneurysm • Uterine pathology (fibroids) • Irritable bowel (SI pain) • Hip pathology
Imaging modalities • Xrays good first line Ix if red flags, osteoporotic fracture • Bone scan (also good initial Ix if Xray nad and red flags) - mets, infection, pagets, PMR • CT Scan bone tumours fractures and spinal stenosis • MRI spinal cord, nerve roots, discs, haemorrhage • Dexa Scan Bone density
TREATMENTS Simple Back Pain (over 95% of cases) Aim: to relieve symptoms and mobilise early. Avoid Bed rest Paracetamol (+nsaid if insufficient) Avoid opiates if at all possible No evidence that co-analgesics better than paracetamol alone. Muscle relaxants (diazepam / methocarbamol) small additional benefit.
No evidence for: • Short wave diathermy • TENS • Spinal manipulation • Traction • Acupuncture • Exercises • Spinal cortisone injections
Occupational issues • More sick leave : Less chance of recovery • 4-12 w - 40% chance of still being off at 1 year. • Don’t need to be pain free to return to work • MDT Rehabilitation programs: psychological therapies; CBT; graduated return to work (light duties)
Blocks to returning to work (blue flags!) • perceived work load • low pay • management attitudes • poor support • loss of confidence • depression
JD’s top tips for back pain. • Patient who attends a second time with “simple” back pain- get them to strip to their underwear!
Top tips • True sciatica means that the leg pain is worse than the back pain- start examination with them sitting on the couch.
Top tips • With radiculopathy re-examine regularly, carefully note findings and refer early if weakness (foot drop can be irreversible)
Top Tips • Physios are very good at managing the psychological aspects of chronic pain.
Top Tips • Sending someone to casualty is pointless but can have a very useful ‘placebo’ effect in showing the patient how impressed you are with his or her pain.