Download
1 / 36
380 likes | 563 Views
George A. Beller MD, MACC, FACP Ruth C. Heede Professor of Cardiology and Professor of Medicine, Chief of the Cardiovascular Division University of Virginia Health System Charlottesville, Virginia. Radionuclide Versus Other Evidence For a Mechanism of Action. Exercise Results*. 50. Sham.

E N D
George A. Beller MD, MACC, FACPRuth C. Heede Professor of Cardiology and Professor of Medicine, Chief of the Cardiovascular DivisionUniversity of Virginia Health SystemCharlottesville, Virginia Radionuclide Versus Other Evidence For a Mechanism of Action
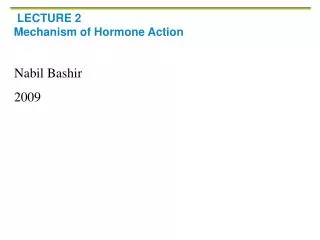
Exercise Results* 50 Sham Active 42 p > 0.3 37 40 p = 0.01 30 26 20 Time (Seconds) 10 -4 0 Exercise Duration Time to ST Depression -10 *Adjusted mean of change from baseline (Arora RR, et al. J Am Coll Cardiol 1999;33:1833-40) MUST-EECP
Mechanism For Sustained Clinical Benefit With EECP • Mechanism remains undefined. • Potential mechanisms include: • Recruitment of coronary collaterals. • Angiogenesis. • Improved endothelial function. • Training effect. • Other, yet unknown mechanism (s).
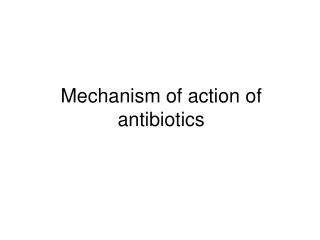
EECP Effect on Radionuclide Stress Perfusion Stress Rest Pre-EECP Stress Rest Post-EECP (Lawson, Hui:J Critical Illness.2000;15(11):629-636)
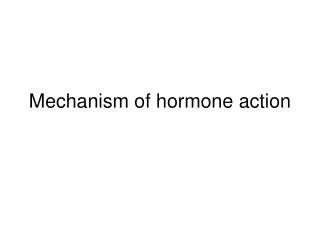
Prevalence And Type of Perfusion Abnormalities Before And After EECP Treatment *p<0.01 vs before EECP treatment (Urano H, Ikeda H, et al. JACC 2001;37:93-99)
Effect of EECP on Myocardial Perfusion in Patients with Stable CAD: a Pilot Study • Clinical Sites • UCSD A Demaria, A Raisinghani • UVA G Beller, I Sarembock • U Florida CR Conti • UCSF A Michaels • UPMC A Feldman, O Soran • Mayo Clinic G Barsness • Core Laboratories • UVA D Watson (Radionuclide) • Cornell P Kligfield (Exercise) • Coordinating Center • Anabase P-A de Lame, M Lemaire
Purpose • Using blinded core laboratories for analyses of nuclear myocardial perfusion and exercise ECG data, we assessed changes in exercise-induced myocardial ischemia after 35-hours of EECP.
Revascularization 1Perfusion Pre Treatment Post Treatment
Inclusion Criteria • Class II-IV refractory stable angina. • Able to exercise at least 3 minutes on the Cornell treadmill protocol. • Presence of at least one target segment defined as a reversible perfusion defect on technetium-99m-sestamibi SPECT exercise perfusion imaging, confirmed by core laboratory.
Study Protocol • 35-hour course of EECP. • Prior to and 1-month after EECP: • Initial exercise tests were repeated once at one-week interval. • Symptom-limited quantitative gated technetium-99m-sestamibi SPECT exercise perfusion imaging (sestamibi injected at same HR in both stress tests). • QOL: SF-36 and Seattle Angina Questionnaire (SAQ).
Baseline Demographics Patients enrolled 37 Patients evaluable 34 Age (years) ± SD 61 ± 10 Male 81% BMI 28.7 ± 6.3 Hyperlipidemia 92% Diabetes mellitus 49%
Baseline CAD Factors Prior myocardial infarction 70% Multivessel disease 92% LVEF ± SD 55 ± 9% Prior PCI 54% Prior CABG 66% Prior myocardial laser revasc 9%
Baseline Angina Class Angina class I 0% II 38% III 49% IV 13%
Exercise Treadmill Test Results • Pre-EECP • 71% had angina during ETT • Post-EECP • Of those with angina on pre-EECP ETT, 54% also had angina during post-EECP ETT. • 12% in exercise duration. • 65% angina-free exercise duration.
Radionuclide Imaging Methods • Target segments were assessed by the core laboratory independent of the sequence of the test (baseline or follow-up). • SPECT images were obtained at rest and stress. • Qualitative and quantitative assessments were performed, providing measures of defect magnitude and reversibility. • Thickening fraction was used to assess segmental systolic function pre- and post-EECP treatment.
Quantitative SPECT: Stress, Target Segments Baseline Follow-up Change %Change Mean 63.4% 62.9% -0.5 -0.8 S.D. 11.6 13.3 6.7 11.9 N 34 p=value 0.66 NS
Quantitative SPECT: Rest, Target Segments Baseline Follow-up Change %Change Mean 73.9% 72.6% -1.3 -1.4 S.D. 10.7 9.9 5.5 7.8 N 34 p=value 0.17 NS
Quantitative SPECT: Magnitude of Reversibility Baseline Follow-up Change %Change Mean 10.5% 9.6% -0.8 4.3 S.D. 6.4 7.9 7.2 82.6 N 34 p=value 0.51 NS
Quantitative SPECT: Thickening Fraction Baseline Follow-up Change %Change Mean 27.3% 27.6% 0.3 14.5 S.D. 11.4 13.5 10.3 94.2 N 32 p=value 0.87 NS
Quantitative SPECT: Left Ventricular Ejection Fraction Baseline Follow-up Change %Change Mean 55.3% 54.1% -0.8 -0.5 S.D. 8.8 9.2 8.0 16 N 33 p=value 0.56 NS
130801 Perfusion Pre Treatment Post Treatment
Angina Class 100% 80% 4 60% 3 2 40% 1 20% 0% Baseline 1-mo Follow-up
QOL Improvement Post-EECP SF-36 Questionnaire Category % Improvement P-Value General health perceptions 52 0.002 Physical limitations 74 <0.001 Emotional limitations 4 0.057 Social functioning 73 <0.001 Bodily pain 68 <0.001 Mental health 18 0.02 Vitality 97 <0.001
QOL Improvement Post-EECP Seattle Angina Questionnaire Category % Improvement P-value Exertional capacity 84 0.003 Anginal stability 74 <0.001 Anginal frequency 75 <0.001 Treatment satisfaction 26 <0.001 Disease perception 108 <0.001
Conclusions • We confirm that EECP reduces angina, improves exercise capacity, and improves QOL. • There were no significant changes in mean defect magnitude, amount of reversibility, or thickening fractions on SPECT imaging when compared at identical pre- and post-EECP heart rates. • Potential mechanisms of benefit with EECP include improved endothelial function and a training effect.
Limitations • SPECT records relative changes in myocardial perfusion. In order to detect an absolute change in overall myocardial perfusion, PET imaging would be required.
Effects of EECP on ANG II Activity p<0.05 p<0.05 Tissue (pg/gm w w) 2000 Control AMI AMI+EECP * 1800 * p<0.05 vs Control † p<0.05 vs AMI 1600 1400 1200 *† * 1000 * *† 800 † 600 400 * *† 200 0 Plasma Heart Aorta Kidney Lung Dog model data --- Presented at the Heart Failure Society of America, Washington Sept 11, 2001
120 96.37 100 76.57 78.44 80 62.06 57.52 60 44.45 35.15 40 20 0 Change in Plasma Endothelin/Nitric Oxide Ratio Pre-EECP During EECP (1 hour/d) Post-EECP -- P ≤0.05 -- -- P ≤0.01-- P ≤0.05 Endothelin/nitric oxide ratio Control After 1 Hr After 12 Hr After 24 Hr After 36 Hr After 1 Mo After 3 Mo (Wu GF, et al. Circulation 1999;100(18)I-832(#4390))
160 140 120 107.9 100 75.8 80 53.7 49.9 60 40 20 0 Control Day 1 After 1 wk After 1 mo Effect of EECP Therapy on Nitric Oxide * P < 0.01 vs baseline * Plasma Nitric Oxide (mol) (Masuda D, Nohara R, et al. Eur Heart J 2001;22(16):1451-58)
120 105.47 91.15 100 87.1 80 70.86 63.36 60 48.52 40.78 38.88 40 20 0 Effect of EECP on NO Nitric Oxide (mol/L) Pre- 1 h 12 h 24 h 36 hr Pre- 6 wk Control EECP Treatment Medical Therapy (Qian XX, et al. J Heart Dis 1999;1:1193(769))
Factor % of Patients with increase HGF 66.6% bFGF 66.6% MCP-1 33.3% VEGF 33.3% EECP Change in Angiogenic Factors 26.6 30 25 18.8 20 15.6 Increase (%) 15 10 5 0 0 HGF bFGF VEGF MCP-1 (Masuda D, et al. Circulation 2001;104(17) Suppl II:444(2109))
25 20 15 10 5 0 Baseline 1 Hour 17 Hours 35 Hours 1 Week I Month Influence of EECP on Serum VEGF During EECP After EECP Increase in Serum VEGF From Baseline (%) (Kho, Liuzzo, Suresh K. Endocrine Society’s 82nd Annual Meeting 2000, 6/21-24, Toronto, Canada )
Conclusions: Possible EECP Mechanisms • Improvement in endothelial function reflected by increase in organ blood flow, increased NO and decreased endothelin • Decreased oxidative stress and decreased angiotensin II production • Coronary collateral recruitment and development; arteriogenesis and angiogenesis (increased VEGF levels) • Peripheral training effect permitting longer exercise time with less ischemia
Comment The mechanism of benefit of EECP does not appear to be related to an improvement in exercise induced ischemic perfusion defects. Thus, enhanced collateral blood flow to ischemic zones may not occur.