Weekly Symptom Variability in Sexually Abused Youth: Treatment Needs and Responses
This study investigates the weekly symptom variability in sexually abused youth undergoing treatment, with a focus on how varying levels of presenting symptomatology (low, medium, high) influence symptom changes across several areas, including mood, behavior, and emotional communication. By collecting weekly reports, the research provides insight into the subtle changes in symptom presentation throughout treatment, highlighting the differences in symptom severity and the effectiveness of interventions for groups categorized as low, at-risk, or clinically significant.

Weekly Symptom Variability in Sexually Abused Youth: Treatment Needs and Responses
E N D
Presentation Transcript
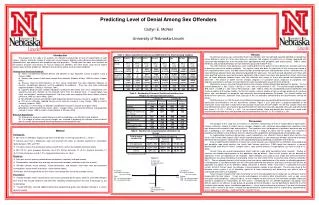
Weekly Symptom Variability in Sexually Abused Youth Undergoing Treatment: The Needs and Responses of Youth with Various Levels of Presenting Symptomatology Genelle K. Sawyer and David J. Hansen University of Nebraska-Lincoln Introduction Results Sexually abused children and adolescents display a considerable breadth of symptoms, including anxiety, depression, sexualized behavior, low self-esteem, post-traumatic stress symptoms, and behavioral problems (e.g., Kendall-Tackett, Williams, & Finkelhor, 1993). However, such victimization does not necessarily have an inevitable pattern or a unified symptom presentation for the majority of youth. Rather, sexually abused youth display a multitude of patterns of symptoms at varying levels of severity ranging from asymptomatic to clinically significant in multiple areas of functioning. Given the complexity of symptom presentation for sexually abused youth and the sensitive and intrusive nature of sexual abuse and its related topics, researchers have sought to determine the general benefits of different types of treatment as well as who is most likely to benefit from the treatment. To date, the majority of treatment outcome studies have relied on comprehensive assessments conducted at pre- and post-treatment (e.g., Cohen & Mannarino, 1996a; Cohen & Mannarino, 1998; Deblinger, Stauffer, & Steer, 2001) and have, therefore, been unable to monitor the weekly progress of the child or to determine specific gains or losses in symptomatology through the course of treatment. In addition, researchers are posed with the dilemma of asymptomatic youth: should these youth be in treatment when they are demonstrating no signs of maladjustment? The purpose of the present study was to examine how varying levels of presenting symptomatology for youth at pre-treatment (e.g., low, medium, high) influence weekly symptom presentation across a variety of areas (e.g., negative moods, problems behaviors, interpersonal interactions, abuse related emotional and communication problems) throughout treatment. Obtaining weekly reports of symptomatology throughout treatment allows for a unique look at the subtle changes experienced on a weekly basis. Table 1: Univariate Statistics Descriptive Statistics: Based on pre-treatment scores on the CBCL Total Problems Scale, participants were placed into groups representing varying levels of presenting symptomatology (i.e., Low equals a score of less than 60 on the CBCL, At-risk a score between 60 and 69, and Clinically Significant a score of greater than 70). Participants were divided fairly evenly between groups with 30 participants in the Low group, 35 in the At-risk group, and 25 in the Clinically Significant group. Descriptive statistics for weekly scores on the Weekly Problems Scales by group are presented in Table 1. Additionally, weekly means for the WPS-C and WPS-P are depicted graphically in Figures 1 and 2, respectively. On both the WPS-C and WPS-P, trends were as expected with the Clinically Significant group demonstrating higher levels of problems and the Low group the lowest level of problems; however, each group appeared to decrease in symptomatology over the course of treatment. Similar trends were found in each of the subscales on the WPS-C (i.e., Negative Moods and Behaviors and Self-Esteem Problems) and WPS-P (i.e., Problem Behaviors, Negative Moods, and Sex and Sexual Abuse Communication Issues) with one exception on each scale. On the WPS-C Problem Peer and Parental Interactions Subscale the Low group appeared to demonstrate little change, while the At-risk and Clinically Significant groups appeared to decrease in problems over the course of treatment. Similarly, on the WPS-P Problem Family and Parenting Subscale, the Low and At-risk groups appeared to demonstrate little overall change, while the Clinically Significant group decreased in problems over the course of treatment. Repeated Measures ANOVAs: To test these results statistically, Mixed Groups Factorial ANOVAs were conducted to determine if there are significant differences on the Weekly Problems Scales between and within groups over the course of treatment (See Table 2). For purposes of the analyses, three-session intervals were created to simplify the process for the 12 sessions of treatment. Averages were computed for weeks 1-3, 4-6, 7-9, and 10-12 of treatment (See Tables 3 and 4). Due to missing data, analyses for the WPS-C include 60 participants and 58 participants for the WPS-P. Looking first at the WPS-C, there was a main effect over time for WPS-C Weekly Totals (F(3,171) = 10.92, p < .001), with WPS-C Totals decreasing over the course of treatment for all three symptomatology groups. However, there were no significant differences between symptomatology groups. On the WPS-P, there was a main effect over time for WPS-P Weekly Totals (F(3, 165) = 3.19, p < .05), with WPS-C Totals decreasing over the course of treatment, however, this pattern is only descriptive of the Clinically Significant group. There was also a main effect for CBCL Total Groups (F(2,55) = 5.70, p < .01). Results indicate that at the beginning of treatment there is a significant difference between the Clinically Significant group and the Low group, however, these results are no longer descriptive as treatment progresses. Table 2: Summary of Mixed Groups Factorial ANOVA for WPS Weekly Scores and CBCL Total Groups Method • Participants: • Participants included 90 youth and their nonoffending caregivers who completed Project SAFE, a 12-session cognitive-behavioral group treatment (e.g., Hansen, Hecht, & Futa, 1998; Hsu, 2003). Of the nonoffending parents, the mean age was 36.94 (SD = 6.51; range of 23 to 60). Sixty-two (72.1%) of the caregivers were the biological mother. The vast majority (91.8%) identified themselves as Caucasian. The sample was predominately lower to lower-middle class and approximately half were married. • The children ranged in age from 6.05 to 16.33 years with a mean age of 11.15 years (SD = 3.03). Fifty-one (80%) of the youth were female and 77.8% were Caucasian. Most of the victims were abused by only one perpetrator (86.7%) and the majority of the offenders were non-family members (53.3%). Only two children experienced non-contact forms of abuse (i.e., exposure, pornography) and the most common type of sexual abuse behaviors identified in this sample was fondling (71.1%). • Measures: • Children completed the Weekly Problems Scale-Child Version (WPS-C) and caregivers completed the Weekly Problems Scale-Parent Version (WPS-P) as well as the Child Behavior Checklist – Parent Report Form (CBCL; Achenbach, 1991). The Weekly Problems Scales were developed by Project SAFE researchers to provide a brief, efficient means of assessing multiple domains of child functioning and have been found to demonstrate good internal consistency, temporal stability, and construct validity (Sawyer, Tsao, Hansen, Flood, 2004). • Weekly Problems Scale-Child Version (WPS-C; Sawyer, Futa, Hecht, & Hansen, 2004). The WPS-C consisted of 11 statements (e.g., “I feel sad,” “I get along with my friends”) and children are asked to mark one of six responses (i.e., never, almost never, a little of the time, some of the time, most of the time, all of the time) that best describes their feelings and interactions during the past week. • Weekly Problems Scale-Parent Version (WPS-P; Sawyer, et al, 2004). The WPS-P consisted of 15 statements (e.g., “During the past 7 days my child appeared unhappy, sad, or depressed”). Parents are asked to rate each statement on a scale from 1 (never) to 10 (always). • Procedures: • All participants completed an initial comprehensive assessment consisting of the above measures prior to treatment. Caregivers and children completed the Weekly Problems Scales (i.e., WPS-C and WPS-P) at each session throughout the course of the 12-week treatment. Table 3: Mean Scores of WPS-C Weekly Total Scores as a Function of CBCL Total Group Table 4: Mean Scores of WPS-P Weekly Total Scores as a Function of CBCL Total Group Discussion Figure 1: WPS-C Weekly Totals Over the Course of Treatment The purpose of the present study was to examine how varying levels of presenting symptomatology for youth at pre-treatment influence weekly symptom presentation across a variety of areas over the course of treatment. Overall, results indicate that, while there are many similarities among groups, the level of symptomatology a youth presents with may influence their treatment experience. Youth reported a decrease in symptomatology over the course of treatment for all symptomatology level groups, however, parents reported a significant decrease for only the Clinically Significant group. Additionally, youth appear more diverse in their presentation at the beginning of treatment with the gap closing as treatment progresses, according to parent report. Additionally, this study provides a unique look at the experience of asymptomatic youth over treatment. A debate exists in the literature about the potential benefits or detriments of routinely providing treatment to those children who display few to no symptoms after sexual abuse. Results of this study indicate that asymptomatic children experienced a slight decrease in symptomatology over the course of treatment, suggesting that even children who present with few symptoms can make gains in treatment and are not harmed by their inclusion in treatment with symptomatic children. Additionally, it is likely that they will continue to benefit from the psychoeducational and prevention aspects of the treatment in the future. Limitations of this study include the small sample size as well as the loss of participants in the analyses due to missing data. Future research should attempt to use longitudinal data analyses which will allow those participants with missing data to remain in the sample. Figure 2: WPS-P Weekly Totals Over the Course of Treatment