Download
1 / 26
380 likes | 909 Views
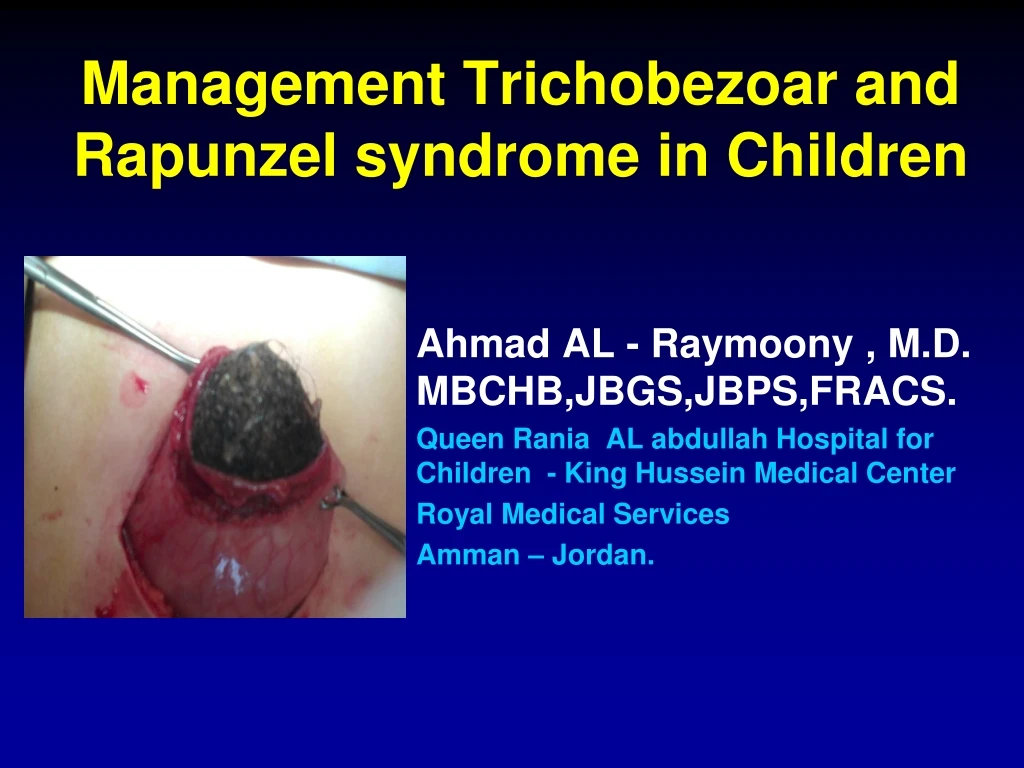
Management Trichobezoar and Rapunzel syndrome in Children. Ahmad AL - Raymoony , M.D. MBCHB,JBGS,JBPS,FRACS. Queen Rania AL abdullah Hospital for Children - King Hussein Medical Center Royal Medical Services Amman – Jordan. Queen Rania Aladullah Hospital for Children.

E N D
Management Trichobezoar and Rapunzel syndrome in Children Ahmad AL - Raymoony , M.D. MBCHB,JBGS,JBPS,FRACS. Queen Rania AL abdullah Hospital for Children - King Hussein Medical Center Royal Medical Services Amman – Jordan.
Trichobezoar: Background • Trichobezoar, a hair ball in the proximal gastrointestinal tract . • Uncommon in children, • almost exclusively seen in young females .
Trichobezoar : PATHOGENESIS • Human hair is resistant to digestion as well as peristalsis due to its smooth surface. Therefore it accumulates between the mucosal folds of the stomach. • Over a period of time, continuous ingestion of hair leads to the impaction of hair together with mucus and food, causing the formation of a trichobezoar.
Where does it occurs? • In most cases the trichobezoar is confined within the stomach. In some cases, however, the trichobezoar extends through the pylorus into jejunum, ileum or even colon. This condition called Rapunzel syndrome • first described by Vaughan et al. in 1968. • Incidentally, parts of the tail can break off and migrate to the small intestine, causing intestinal obstruction.
Trichobezoars: clinic presentation • In the early stage, most trichobezoars may not be recognized due to their nonspecific presentation or even lack of symptoms . • One should be aware of a trichobezoar in young females with psychiatric comorbidity, as it is usually the result of the urge to pull out one’s own hair (trichotillomania) and swallow it (trichophagia).
Trichobezoars : clinic presentation • Other psychiatric disorders, however, such as • mental disorders, abuse, pica, obsessive compulsive disorder, depression and anorexia nervos. • may also be associated with trichobezoar .
Trichobezoars : Complications • Reported complication in literature • Intussusception, obstructive jaundice, protein-losing enteropathy, pancreatitis and even death. • Gastric mucosal erosion, ulceration and even perforation of the stomach or the small intestine.
trichobezoars: Managements • In the literature several treatment options are proposed : • Conventional laparotomy. • Laparoscopy. • Endoscopy. • Conventional laparotomy is still the treatment of choiceespecially forRapunzel syndrome.
Trichobezoars The aim of this study is to evaluate our experience in the management of trichobezoar in children.. Between february 2009 and june 2012, five patients have been treated for trichobezoar in our unit. their charts were reviewed with respect to clinical presentation, diagnostic procedures, surgical treatment and postoperative follow up.
Trichobezoars : clinical presentation chronic abdominal pain, vomiting , weight loss, epigastric fullness, alopecia.
Trichobezoars:Investigations In all our patients plain abdomen x-ray, abdomen u/s, and upper gastrointestinal series were performed. One of our patients was diagnosed as case of intussusception, only in two of them endoscopic diagnosis of trichobezoar were done.
Trichobezoars: Surgical Results • All of them were treated by conventional laparotomy, and complete evacuation of hair ball were done. • all of them were females. • median age at the time of surgery was 12 ( range 4-15) years. • The location of the hair ball was in the stomach in 3 patients, and in the stomach and small bowel in 2 patients ( rapunzel syndrome).
Trichobezoars: Follow-Up • All of our patients eventually proved to suffer from trichophagia and referred to a child psychatrist. • All patients are are free of symptoms • No recurrence have been reported.
Conclusions • Trichobezoar should be considered in young females presenting with recurrent non specific abdominal pain and epigastric fullness. • Endoscopy can be used as one of the diagnostic modalities. • Psychartric consultation is necessary to prevent relapse.
Conclusions • . • Conventional laporatomy is the treatment of choice in children with tichobezoar . • the only valid management for rapunzel syndrome.