Download
1 / 22
220 likes | 367 Views
Incorporating Time to Death into Medicare FFS A+B Projections. Liming Cai, Ph.D Andrew Madison Office of the Actuary Centers for Medicare and Medicaid Services Middle Atlantic Actuarial Club Annual Meeting September 13, 2012. Outline. The age-sex adjustment

E N D
Incorporating Time to Death into Medicare FFS A+B Projections Liming Cai, Ph.D Andrew Madison Office of the Actuary Centers for Medicare and Medicaid Services Middle Atlantic Actuarial Club Annual Meeting September 13, 2012
Outline • The age-sex adjustment • The age-sex-time to death (TTD) adjustment • Data • Methods • Results • Conclusion • Discussion
Medicare FFS Spending Projection • Medicare FFS population • Per capita FFS spending • Short run • Demographics • Price updates • Residuals • Long run • Demographics • Residuals
The Demographic Adjustment by Age and Sex • Calculate average spending for 65+ by sex and 5-year age groups (except for 85+) relative to average spending for all 65+ over a three-year base period (2008-2010) • For each of the next 75 years, multiply the fixed relative spending estimates by the age distribution of beneficiaries to derive weighted average relative spending • Multiply this relative spending by average spending in a base year (2010 for TR 2012) and the number of beneficiaries in the year for which spending is projected to derive total Medicare spending projections
Assumptions and Implications of the Age-Sex Adjustment • Assumes future 85+ as expensive as today’s 85+, holding everything else constant • Total spending is driven by the age-sex distribution of future beneficiaries only • As mortality rates fall and people live longer, there are more expensive elderly, and hence higher spending
Average AB Spending Varies by Age Source: CMS 100% claims file. FFS AB spending on aged-in benes only.
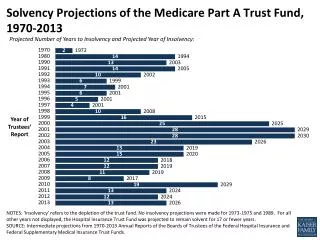
Why Are 85+ More Costly? • Closer to death – demographic reason 2012 mortality rate at ages 65-119 (SSA TR2012)
Why Are 85+ More Costly? • End of life care is expensive – non-demographic reason • Recent OACT study, Riley and Lubitz (2010, HSR) – 25-30% stable since 1970s
Calculation of Avg. Spending at Age t • Average spending at age t can be calculated as i.e., the sum of the product of avg. spending at year i before death and the dist. of time to death. • Example: Avg. spending for 85-year old men=$25K Constant age-specific spending implies fixed time to death distributions at age t.
SSA TR2012 Projection – Life Expectancy Men Women Source: SSA TR2012 intermediate projections.
SSA TR2012 Projection - Time to Death Source: SSA TR2012 intermediate projections.
The Age-Sex-TTD Adjustment • Adds a 3rd dimension • Spending by TTD, age group, sex and year • TTD distribution by age group, sex and year • Number of beneficiaries by age group, sex and year • Recognizes that • Higher proportion of 85+ is caused by shifts in TTD dist. • Shifts in TTD dist. imply that future 85+ are not as expensive as today’s 85+, holding everything else constant • TTD is not the same concept as population health • Technical Panel in 2000 recommended distinguishing between decedents and survivors • CBO has incorporated TTD into CBOLT
Data • The IDR 100% sample of beneficiary claims in 2011 • 1.2 million decedents in 2011 among 28 million “aged-in” benes age 65-115 with equal A & B exposure months. 5.9 million observations of spending of up to 4 years before death • Decedents’ spending in 2007-2010 are inflated to 2011 dollar using OACT’s personal health care spending index • 5 age groups: 65-69, 70-74, 75-79, 80-84, 85+ • Average spending in TTD=0,1,2,3,4+ weighted by member months, consistent with the age-sex method • Decedents’ spending in TTD=0 is actual 2011 $, NOT last-12 mo $ • Average (exposure-weighted) spending in TTD=4+ is calculated using 2007 spending for all 2011 benes because of large spending differentials in 2007 between decedents and survivors.
Average Spending by Time To Death for 2011 Decedents Source: IDR 2011 FFS AB decedents.
Projection of FFS AB Spending in 2012-2087 • The age-sex method • Relative spending ratios in baseline (2011), by age group and sex, are multiplied by average spending in 2011 ($10,059 for men and $10,084 for women), and the number of beneficiaries in 2012-2087 in the corresponding age group and sex cells • The age-sex-TTD method • Theoretical TTD distributions for 2012-2087, by age group and sex • Estimated from SSA TR2012 intermediate life tables using microsimulation • Average spending of 2011 decedents by age group, sex and TTD are multiplied by the number of beneficiaries in the corresponding age group, sex and TTD cells • A set of adjustment factors, by sex and age groups, is applied to ensure that projected 2011 spending are equal for both methods. Unadjusted difference in 2011 spending is 7% or less due to imperfect information in 2012
Projection Results Age-Sex Note: Calculation based on 2007-2011 IDR data and SSA TR2012 intermediate projections.
Projection Results Note: Calculation based on 2007-2011 IDR data and SSA TR2012 intermediate projections.
Conclusion • The age-sex-TTD method projects lower Medicare spending than the current age-sex method • The age-sex-TTD adjustment • Consistent with all SSA demographic assumptions • Sets the lower bound of projection
Will the Pattern of Spending by TTD Change? • This stable historical pattern reflects two fundamental principles • What is going to change? • Shape – Immortality? Death panel? The answer is No. • Level – Very likely due to a variety of factors, which is not part of demographic adjustment and, more importantly, will affect both methods equally.
Remaining Issues • Next steps • Separate analysis by types of service – will allow unequal number of enrollees for A & B services. In this preliminary analysis Parts A & B enrollees are assumed equal. • Under 65-year olds? • The endogeneity of TTD distributions • Per capita health spending growth will impact future TTD distributions • SSA projections may have underestimated the negative impact, resulting in overly optimistic projections of future mortality improvement
What Kills Us Source: Death in the US, 2010. NCHS Data Brief, June 2012