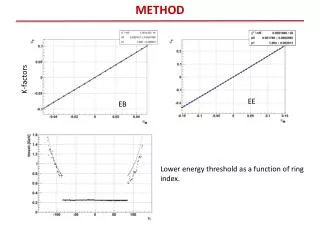
METHOD
Long-Term Neuropsychological Functioning Following Mild Traumatic Brain Injury Nathalie C. B é rard and Dennis P. Alfano. INTRODUCTION

METHOD
E N D
Presentation Transcript
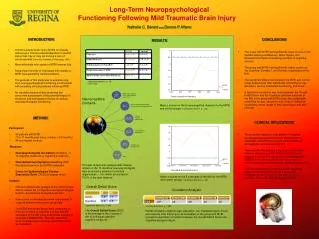
Long-Term Neuropsychological Functioning Following Mild Traumatic Brain Injury Nathalie C. Bérardand Dennis P. Alfano • INTRODUCTION • A mild traumatic brain injury (MTBI) is clinically defined as a “trauma induced alteration in mental status that may or may not involve a loss of consciousness” (American Academy of Neurology, 1997) • Most individuals who sustain a MTBI recover fully • A significant minority of individuals who sustain a MTBI have persisting clinical problems. • The purpose of this study was to examine long- term neuropsychological functioning in individuals with persisting clinical problems following MTBI • An important feature of this study was the concurrent assessment of the potential impact of emotional and demographic factors on clinical neuropsychological functioning • RESULTS CONCLUSIONS • The group with MTBI had significantly lower scores on the Verbal Learning and Memory, Motor Speed, and Speeded Information Processing domains of cognitive function • The group with MTBI had significantly higher scores on the Cognitive, Somatic I, and Somatic II subscales of the NSI • The significant differences between the MTBI and control group existed even after statistically controlling for age, education, level of intellectual functioning, and mood • A significant correlation was found between the Overall Deficit Score and the Cognitive symptom subscale of the NSI in the group with MTBI (even after statistically controlling for age, education, sex, level of intellectual functioning, mood, length of time since injury, and pain severity) • CLINICAL IMPLICATIONS • These results indicate a clear pattern of impaired neuropsychological functions over the long-term in individuals with MTBI that occurs independently of demographic and emotional factors • These results also indicate a significant relationship between objective cognitive deficits and increased symptoms of cognitive dysfunction in individuals with MTBI that occurs independently of demographic, emotional and pain-related factors, and time since injury • The clinical treatment of individuals with persisting problems following MTBI should therefore be multidimensional and incorporate intervention for cognitive, emotional, and somatic dysfunction *significantly different, p < .05 **mean (SD) Neurocognitive Domains • Grooved Pegboard Dominant • Grooved Pegboard NonDominant Mean z scores on the 6 neurocognitive domains for the MTBI and control groups (*significantly different, p < .05) • METHOD • Trails A • Trails B • Digit Symbol • Participants • 92 patients with MTBI • (1 to 71 months post-injury; median = 9.5 months) • 94 non-injured controls • Measures • Neuropsychological test battery consisting of 13 objective measures of cognitive functioning • Neurobehavioural Symptom Inventory (NSI)that tapped common post-MTBI symptoms • Centre for Epidemiological Studies Depression Scale (CESD) to assess mood • Analysis • Principal components analysis of the control group data to reduce the 13 objective neuropsychological tests to core domains of cognitive function • Raw scores on all measures were transformed to z scores based on the control group data • The MTBI and control group were compared on the core domains of cognitive function and the subscales of the NSI using multivariate analysis of covariance (MANCOVA), with age, education, level of intellectual functioning, and CESD score as covariates. • FAS Principal components analysis with varimax rotation of the 13 objective neuropsychological tests produced a solution of 6 factors (eigenvalues > 1.0), which accounted for 79.5% of the total variance Mean z scores on the 5 subscales of the NSI for the MTBI and control groups (*significantly different, p < .05) Overall Deficit Score Correlation Analysis *significantly different, p < .005 The Overall Deficit Score (ODS) is the average of the z scores of the 13 individual objective cognitive measures *significantly different, p < .005 Partial correlation analysis (age, education, sex, intellectual level, mood, pain severity, time since injury as covariates) in the group with MTBI revealed a significant correlation between the Overall Deficit Score and Cognitive symptom report