1 / 41
410 likes | 428 Views
A healthy immune system defends the body against disease and infection. But if the immune system malfunctions, it mistakenly attacks healthy cells, tissues, and organs. Called autoimmune disease, these attacks can affect any part of the body, weakening bodily function and even turning life-threatening.

E N D
In an autoimmune disease or autoimmunity, the immune system fails to display self-tolerance and attacks the person’s own tissues. • Autoimmune diseases usually arise in early adulthood and are common, afflicting an estimated 5% of adults in North America and Europe. • Females suffer autoimmune diseases twice as often as males. • Recall that self-reactive B cells and T cells normally are deleted or undergo during negative selection.
A variety of mechanisms produce different autoimmune diseases. • Some involve production of autoantibodies, antibodies that bind to and stimulate or block self-antigens. • For example, autoantibodies that mimic TSH (thyroid-stimulating hormone) are present in Graves disease and stimulate secretion of thyroid hormones (thus producing hyperthyroidism); autoantibodies that bind to and block acetylcholine receptors cause the muscle weakness characteristic of myasthenia gravis.
Other autoimmune diseases involve activation of cytotoxic T cells that destroy certain body cells. • Examples include type 1 diabetes mellitus, in which T cells attack the insulin-producing pancreatic beta cells, and multiple sclerosis (MS), in which T cells attack myelin sheaths around axons of neurons. • Other autoimmune disorders include rheumatoid arthritis (RA), systemic lupus erythematosus (SLE), rheumatic fever, hemolytic and pernicious anemias, Addison’s disease, Hashimoto’s thyroiditis, and ulcerative colitis.
Systemic lupus erythematosus • Systemic lupus erythematosus or SLE, or simply lupus (lupus wolf ) is a chronic autoimmune, inflammatory disease that affects multiple body systems. • Lupus is characterized by periods of active disease and remission; symptoms range from mild to life-threatening. • Lupus most often develops between ages 15 and 44 and is 10–15 times more common in females than males. • It is also 2–3 times more common in African-Americans, Hispanics, Asian-Americans, and Native Americans than in European- Americans. • Although the cause of SLE is not known, both a genetic predisposition to the disease and environmental factors (infections, antibiotics, ultraviolet light, stress, and hormones) may trigger it. • Sex hormones appear to influence the development of SLE. • The disorder often occurs in females who exhibit extremely low levels of androgens.
Signs and symptoms • Signs and symptoms of SLE include joint pain, muscle pain, chest pain with deep breaths, headaches, pale or purple fingers or toes, kidney dysfunction, low blood cell count, nerve or brain dysfunction, slight fever, fatigue, oral ulcers, weight loss, swelling in the legs or around the eyes, enlarged lymph nodes and spleen, photosensitivity, rapid loss of large amounts of scalp hair, and sometimes an eruption across the bridge of the nose and cheeks called a “butterfly rash.”
Two immunological features of SLE are excessive activation of B cells and inappropriate production of autoantibodies against DNA (anti-DNA antibodies) and other components of cellular nuclei such as histone proteins.
Treatment • There is no cure for lupus, but drug therapy can minimize symptoms, reduce inflammation, and forestall flare-ups. The most commonly used lupus medications are pain relievers (nonsteroidal anti-inflammatory drugs such as aspirin and ibuprofen), antimalarial drugs (hydroxychloroquine), and corticosteroids (prednisone and hydrocortisone).
Rheumatoid Arthritis Clinical Signs: • Symptoms include morning stiffness around the joints lasting at least 1 hour, swelling of the soft tissue around three or more joints • Others include swelling of the proximal interphalangeal, metacarpophalangeal, or wrist joints, symetric arthritis, subcutaneous nodules, a positive RF test • Also included is a radiographic evidence of erosion of the joints of the hands, the wrist, or both
Rheumatoid Arthritis • Usually begins with nonspecific symptoms such as fever, malaise, weight loss, and transient joint pain • Stiffness and joint pain that gradually improves during the day are characteristics exhibited by most patients • Joint are involved progressively to larger joints in a symmetric manner from the knees, hips, elbows, shoulders and cervical spine • About 25% of patients have nodules over the bones • Nodules may also be found in the myocardium, pericardium, heart valve, pleural, lungs, spleen, and larynx
Rheumatoid Arthritis Immunologic Findings: • The main immunologic finding is the presence of RF • RF is a 19S Ab directed against the Fc portion of IgG • The Ab is not specific for RA as it is found in other diseases such as scleroderma, Sjogren’s syndrome and B cell lymphoproliferative disorders • It has been suggested that RF may be anti-idiotypic antibodies involved in the regulation of immune response.
Rheumatoid Arthritis • Other auto Abs associated with RA include anticollagen Abs, Abs against cytoskeleton filamentous proteins etc. • These Abs may cause immune complex formation with the activation of complement which contribute to pathogenesis • Joint damage is due to invasion of inflammatory cells such as neutrophils, and macrophages • Proliferation of fibroblast, macrophages, mast cells, and stellar cells result in the formation of a pannus, an organized mass of cells that grow into the joint space
Rheumatoid Arthritis Laboratory Diagnosis of Rheumatoid Arthritis: • Diagnosis is based on a combination of clinical manifestations, radiographic findings and lab tests • Laboratory screening test for RF using sheep red cells or latex particles are available and simple to perform • Quantitative test are also available which involve nephelometry and ELISA techniques • RF is found in other diseases such as syphilis, viral infections, leprosy, chronic liver disease, neoplasm and other inflammatory processes
Rheumatoid Arthritis Treatment: • Treatment include palliatives with rest and nonsteroidal anti-inflammatory drugs like salicylates and ibuprofen • Slow-acting antirheumatic drugs (SAARDS) may also be used to treat the condition • New therapy include the use of monoclonal Abs that target T cells
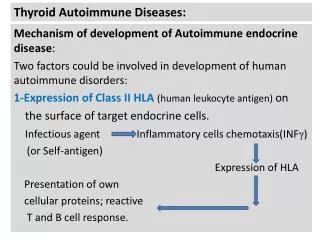
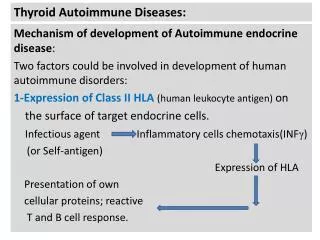
Hashimoto’s Thyroiditis • Hashimoto’s thyroiditis and Graves’ disease are organ specific autoimmune diseases • Both diseases interfere with the thyroid gland function • The thyroid gland located in the anterior region of the neck consist of units called follicles • Follicles are lined with cuboidal epithelial cells and filled with colloid • The primary constituent of colloid is thyroglobulin which is made up of triiodothyronine (T3) thyroxine (T4) • TRH acts on the pituitary gland to induce the release of TSH
Hashimoto’s Thyroiditis • TSH binds to receptors on the cell membrane of the thyroid gland causing break down of thyroglobulin into T3 and T4 • AutoAbs may interfere with this process and cause under or overactivity of the thyroid • Hashimoto’s thyroditis is most often seen in women between the ages of 30 and 40 years • Patients develop a combination of goiter or enlarged thyroid, hypothyroidism and thyroid autoantibodies • An association with HLA antigens DR4 and DR5 has been noted. DQA1 and DQB1 genes seem to confer resistance
Hashimoto’s Thyroiditis Immunologic Findings: • Lymphocytic infiltration is seen with development of germinal centers that almost replace the normal glandular architecture of the thyroid • Cell infiltrates include T and B cells, macrophages and plasma cells • Both CD4 and CD8 cells are found thus the disease is characterized by a cellular and a humoral response • Autoantibodies are found in up to 80% of cases
Hashimoto’s Thyroiditis • Others are thyroid stimulating immunoglobulin (TSI) and thyroid growth-stimulating immunoglobulin (TGSI) • Peroxidase Abs can be measured by particle agglutination assays, complement fixation, RIA and Indirect IFA • Abs to thyroglobulin can be measured by precipitaion in agar, indirect IFA, passive agglutination, RIA, and EIA • Indirect IFA use human or monkey thyroid tissue fixed to a slide • Antithyroglobulin Abs are found in about 80% of patients with the disease
Hashimoto’s Thyroiditis Laboratory Testing: • The autoantibodies present include Abs to thyroglobulin and to thyroid microsomal antigen now known as thyroid peroxidase • Some peroxidase Abs inhibit enzyme activity while others may mediate the cytotoxicity due to natural killer cells • Abs to thyroglobulin help to produce hypothyroid conditions • Other Abs include colloid Ab (CA2) thyrotropin-binding inhibitory immunoglobulin (TBII)
Hashimoto’s Thyroiditis • Others are thyroid stimulating immunoglobulin (TSI) and thyroid growth-stimulating immunoglobulin (TGSI) • Peroxidase Abs can be measured by particle agglutination assays, complement fixation, RIA and Indirect IFA • Abs to thyroglobulin can be measured by precipitation in agar, passive agglutination, RIA, and EIA • Indirect IFA use human or monkey thyroid tissue fixed to a slide • Antithyroglobulin Abs are found in about 80% of patients with the disease
Graves’ Disease • Graves’ disease is another autoimmune disease that affects the thyroid gland • Graves’ disease produces hyperthyroidism • It the most common cause of hyperthyroidism and affects about 0.5% of the population • Women are more susceptible than men by a margin of 7:1 and usually present between the ages of 30 and 40.
Graves’ Disease Clinical Signs: • Disease is presented as thyrotoxicosis with a diffusely enlarged goiter that is soft instead of rubbery • Signs include nervousness, insomnia, depression, weight loss, heat intolerance, sweating, rapid heart beat • Other signs include fatigue, cardiac dysrhythmias, restlessness, and exopthalmus
Graves’ Disease Immunologic Findings: • The thyroid presents with Hyperplasia with a patchy infiltration of lymphocytes • Both CD4 and CD8 cells are present and the T cells appear to play a central role in the pathogenesis of the disease • The most significant Ab present is thyroid stimulating hormone receptor antibody (TRab) • Ag-Ab combination result in the stimulation of the receptor resulting in the release of the thyroid hormones • Another group of Abs called thyroid stimulating antibodies or immunoglobulins (TSab or TSI) may have different specificity
Graves’ Disease Laboratory Diagnosis: • A key finding in Graves’ disease is elevated levels of total and free T3 and T4 • In addition, TSH levels are low due to Ab stimulation of the thyroid • Measurement of the thyroid Abs may be undertaken if the above assays are unclear • Treatment: • Antithyroid medication may be employed. Radioiodine which emits beta particles may be used. Surgery is also an option.
Insulin-Dependent Diabetes • This disease is characterized by insufficient production of insulin due to an autoimmune destruction of the beta cells of the pancreas • Peak onset is b/w 10 and 14 years of age • Disease may be attributed to genetic and environmental conditions • About 95% of white diabetics carry the HLA-DR3 or DR4 genes • It appears that true susceptibility genes for IDDM may occur in the HLA-DQ region
Insulin-Dependent Diabetes • Viral infections have been linked with diabetes • Mumps virus, rubella virus, and Coxsakie B4 virus have all been inconclusively linked to diabetes • Congenital rubella infection is the only one for which a link has been definitively identified • There appears to be similarity between coxsakie viral protein P2-C and the enzyme glutamic acid decarboxylase. • Antibodies are formed against glutamic acid decarboxylase in IDDM • Molecular mimicry could initiate Ab production against self Ag
Insulin-Dependent Diabetes Immunopathology: • Inflammation of the islets of Langerhans in the pancreas leads to fibrosis and destruction of most of the beta cells • CD4 and CD8 B cells and macrophages are all involved in the destructive process of the islet cells • Cellular and humoral immunity are involved in this process • The subset of T cells that is activated determines whether the response is cellular or humoral
Insulin-Dependent Diabetes Laboratory Testing: • IDDM is usually diagnosed by the presence of hyperglycemia • Abs to islet cells may be screened for by indirect IFA with human or rat islet cells • Islet cell may be detected in the sera of newly diagnosed diabetic cases • Abs to insulin may be detected by ELISA or RIA methods
Insulin-Dependent Diabetes Treatment: • Insulin has been the standard form of treatment • New treatment methods center around the use of immunosuppressive agents • Agents that have been tried include azathioprine, cyclosporine A and prednisone • All these agents have potentially toxic effects
Multiple Sclerosis • Destruction of the myelin sheath results in the formation of lesions known as plaques in the white matter of the brain and spinal cord • Genetic and environmental factors predispose one to this disease • MS is associated with the inheritance of HLA antigen DRw15 and DRw6 • An inflammatory response to bacteria or virus may trigger the autoimmune process • Disease is most often seen in those b/w the ages of 20 & 50 and is more common in women
Multiple Sclerosis • 90% of patients alternate between remissions and relapses for many years • Within the plaques, CD4 cells, plasma cells and macrophages are found along with immunoglobulin • Immunoglobulin is increased in the spinal fluid in 60 to 80% of patients • They usually produce oligoclonal bands on protein electrophoresis • RIA is used to detect the Abs • Therapy include use of corticosteroids
Myasthenia Gravis • Symptoms of disease include facial weakness, difficulty in chewing, and swallowing, difficulty breathing • Others include inability to maintain support of the trunk, the neck or the head • Antibody mediated damage to the acetylcholine receptors in the skeletal muscle leads to muscle weakness • May be associated with the presence of other autoimmune diseases such as SLE • Appears to be linked with either HLA-B8 or DRw3 antigens
Myasthenia Gravis • 80 to 90% of patients have Abs to acetylcholine receptors which may be the main contributor to pathogenesis • Combination of the Abs to the receptors blocks the binding of acetylcholine which destroy the receptors • Abs can be detected with RIA methods • Anticholinesterase agents are employed in therapy
Goodpasture’s Syndrome • Goodpasture’s syndrome is a glomerulonephritis due to Abs reacting specifically with Ags in the kidney • Necrosis of the glomerulus is triggered by an Ab that reacts with glycoprotein present in the basement membrane of the glomerulus • Results in immune complex deposit and complement fixation which causes the damage to the kidney • This may eventually produce renal failure
Severe Combined Immunodeficiency (SCID) • The most extreme forms of CID make up a family of disorders termed severe combined immunodeficiency (SCID). • The four general categories of events that have been found to result in SCID include the following:
1. Defective cytokine signaling in T-cell precursors, caused by mutations in certain cytokines, cytokine receptors, or regulatory molecules that control their expression 2. Premature death of the lymphoid lineage due to accumulation of toxic metabolites, caused by defects in the purine metabolism pathways 3. Defective V(D)J rearrangement in developing lymphocytes, caused by mutations in the genes for RAG1 and RAG2, or other proteins involved in the rearrangement process 4. Disruptions in pre-TCR or TCR signaling during development, caused by mutations in tyrosine kinases, adapter molecules, downstream messengers, or transcription factors involved in TCR signaling.
Depending on the underlying genetic defect, an individual with SCID may have a loss of only T cells (TB) or both T and B cells (TB). In either case, both cellular and humoral immunity are either severely depressed or absent. • Clinically, SCID is characterized by a very low number of circulating lymphocytes and a failure to mount immune responses mediated by T cells. • In many cases, the thymus will not fully develop without a sufficient number of T cells, and the few circulating T cells present in some SCID patientsoft en do not respond to stimulation by mitogens, indicating that they cannot proliferate in response to antigens. • In many cases, myeloid and erythroid cells (red-blood-cell precursors) appear normal in number and function, indicating that only lymphoid cells are affected.
Infants born with SCID experience severe recurrent infections that, without early, aggressive treatment, can quickly prove fatal. • Infants with SCID oft en suffer from chronic diarrhea, recurrent respiratory infections, and a general failure to thrive. • The life span of these children can be prolonged by preventing contact with all potentially harmful microorganisms.
If you would like to donate us? Scan below and donate us 0.013$ (US dollar) (5Rs Indian rupee) Contact: If you want PPT/PDF files, please contact below. Email: gnccmysore@gmail.com Telegram:+919738137533(only for Chat)