Urinary System
Urinary System. Marilyn Rose RT, RDMS. outline. Physiology Congenital/ hereditary Inflammatory disorders Urinary Calculi Urinary Tract Obstruction Cysts and tumors Renal Vein Thrombosis Acute renal failure Chronic renal failure. physiology. Kidneys, ureters and bladder

Urinary System
E N D
Presentation Transcript
Urinary System Marilyn Rose RT, RDMS
outline • Physiology • Congenital/ hereditary • Inflammatory disorders • Urinary Calculi • Urinary Tract Obstruction • Cysts and tumors • Renal Vein Thrombosis • Acute renal failure • Chronic renal failure
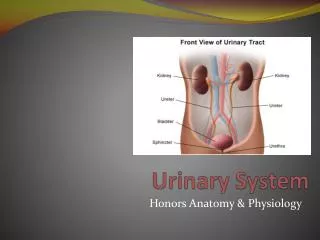
physiology • Kidneys, ureters and bladder • Functional unit- nephron (each kid > 1million) • Filter waste from blood • Reabsorb water and nutrients, secrete excess as urine • Nephron filters 190 L of water each day- only 1-2 L excreted so 99% of water is reabsorbed into the blood. • Urine formation • Begins in glomerulus > BP into Bowman’s capsule allow filtration to occur • Proximal convoluted tubule- lg amt of water and all nutrients are reabsorbed- sodium & chloride depends on {} in the body • Influenced by hormones: antidiuretic (ADH-pituitary) and aldosterone (adrenal glands) • Loop of Henle- reabsorb of salt and water • Distal convoluted- permit excretion of concentrated urine by excreting- potassium & hydrogen ions and some drugs • Kidney maintains salt or electrolyte balance/ acid base balance
Physiology contd. • Healthy metabolism • pH in range of 7.35- 7.45 • < acidic- acid urine > alkaline urine • Urine passes: • collecting tubules-> calyces-> renal pelvis-> ureters • Peristalsis forces urine down ureters • Bladder is a reservoir • Two ureters enter posterior- trigone and anterior corner-urethral opening • 250 ml- stimulate autonomic nerves to void (voluntary contraction of external sphincter- possible if motor system is intact (spinal cord injury- incontinent) • Kidney produces RBC to control blood pressure • Erythropoietin- stimulates rate of production • Renin- produces angiotensin- decreased bloodflow in arterioles increases agniotensin to constrict peripheral arterioles in body causing blood pressure to elevate
Congenital/ Hereditary • Anomalies of: • number/ size • Unilateral renal agenesis (solitary kid) • Rare but associated with other malformations • Failure of embryonic renal bud / vasculature to form • Ureter is also missing • Compensatory hypertrophy of solitary kidney results • Supernumerary kidney • A third small kidney with a separate pelvis/ ureterand blood supply • Can cause 2ndary infections • Hypoplastic kidney • Small replica of a normal kidney- good function • Can also cause compensatory hyperetrophy
Congenital- anomalies • Rotation/ position/ fusion • Ectopic • Pelvic (more common ) • intrathoracic (above diaphragm) (less common) • Usually functions normally but may be more easily obscured • Crossed ectopia • Ectopic kidney lies on the samee side as the normal kidney • Commonly fused with the other kidney • Horseshoe • MOST COMMON TYPE OF FUSION ANOMALY • Both kidneys are malrotated and their lower poles are joined by renal parenchyma (isthmus) across midline • Ureters airseantereiorly and lower pole calyces pint medially • UPJ obstruction is common • Complete fusion • An irregular mass with no resemblance to renal structure “reneform shape”
Congenital- anomalies • Renal pelvis/ ureter • Duplication • Simple bifid pelvis • double pelvis (collecting system) • Complicated by obstruction or VUR • Obstruction usually affects the upper pole • Ureterocele • Cystic dilation of distal ureter near insertion into the bladder • Stenosis leads to prolapse of distal ureter into the bladder • Ectopic ureteroceles are found exclusively in infants and accompanied by ureteral duplication (upper pole obstruction and lower pole VUR) • Radiographic- oval density with a thin halo on US it appears as a cystlike structure within the bladder • Posterior urethral valves • Thin transveerse membranes found in males that cause bladder outlet obstruction and severe hydronephrosis/ hydroureter/ renal damage
Inflammatory Disorders • Glomereulonephritis • Inflammatory process of glomeruli • Antigen-antibody rxn • occurs several weeks post acute respiratory /middle ear infection (hemolytic strep) • More often chronic autoimmune disorder • Leaking into the urine: • albumin (proteinuria) • red blood cells (hematuria) • <glomerular filtration rate = oliguria- < amt of urine • Pyeleonephritis • Inflammation of the kidney and renal pelvis caused by pyogenicbactereia • Affects interstitual tissue between the tubules • Patchy distribution and involves one kidney • Often occurs in women and children • From obstruction- enlarged prostate, kid stone, cong defect) • Catheterization of the ureter • Blunting, round or clubbed calyces • CT and US can also show an abscess, hydronephrosis • Chronic- loss of parenchyma • Emphysematous pyelonephritis • Severe form of acute parenchymal and peerirenal infection with gas-forming bacteria • Occurs in diabetic men • Causes acute necrosis of entire kidney
Inflammatory contd. • TB • Hematogenous spread of TB • Small granulomas in cortex of kids • 2ary infection- 5-10 years post primary • Radiographic- ulcerative destruction of papillae and enlargement of calyces- flecks of ca++ • Papillary necrosis • Destructive process of medullary papillae • Diabetes, pyelonephritis, UTI, sickle cell, phenacetin (acetaminophen) • Radiographic- sloughing of papillae, ca++ • Echogenicnonshadowing structures in collecting system • Cystitis • Inflammation of urinary bladder • More common in women (short urethra)- bacteria • Catheterization- most common nosocomial infection in the hospital • Radiographic- chronic- decreased bladder size, thick wall • Emphysematous in diabetic
Urinary calculi • Most commonly form in the kidney • Asymptomatic until lodge in ureter- partial obstruction • Metabolic abnormality- hypercalcemia (hyperparathyroid) • Also urinary stasis and infection • Radiographic- 80% have enough ca++ to see on xray • Noncon CT demonstrates stone (type), hydroureter or hydronephrosis • US- echogenic, acoustic shadow, hydroureter and hydronephrosis • Staghorn calculi- completely fill pelvis- block urine flow • Nephrocalcinosis- ca++ in parenchyma- hyperparathyroid, sarcoidosis, hyperbvitamin D, ren tub acidosis • Ureter calculi- from downward movement of stone- lodge of UVJ • Bladder stone- elderly men- blad outlet obstrcution, urethral stricture, neuroblad, bladdivertic
UPJ obstruction Urinary tract obstruction • Adults- urinary calculi, pelvic tumor, urethral stricture, enlarged prostate • Children- congenital malformations- UPJ narrow, uretereocele, retrocaval ureter, PUV • Blockage above bladder- unilateral hydroureter and hydronephrosis • Below bladder- bilateral hydroureter and hydronephrosis • Radiographic • CT- mass effects, stone- acute obstruction- kidney swollen • US- detect hydronephrosis • Physiologic hydronephrosis occurs during pregnancy
Renal Cysts • Renal cyst • Simple renal cysts • most common unifocal masses of the kidney • Fluid filled- unilocular (septa occassionally) • Vary in size- single or multiple on one or both kidneys • Some (3%) have a thin calcified wall- not usually in benign • Radiographic- protruding portion elevates the edges of the cortex • US best for distinguishing fluid filled simple cysts (enhancement) from solid lesions • CT also accurate in simple cysts- • Needs to be followed since abscess, necrotic tumors or hemorrhagic cyst can mimic simple cysts
Polycystic kidney disease • Polycystic kidney disease • Inherited disorder (ADPKD) • Multiple cysts of varying size • Lobulated enlargement of kids and progressive renal impairment • Cystic compression of nephrons- • intrarenal obstruction/ HTN • 1/3 -cysts on liver (does not interfere with hepatic function) • 10% -berry aneurysms- cerebral arteries • Asymptomatic during first 3 decades • Radiographic- enlarged kidneys, with multiple varying sized cysts • Renal parenchyma hyperechoic • small cyst that -not fluid filled- wall interface makes them echogeneic • Demonstration of hepatic cysts can make the diagnosis • Screen other family members • Fatal form- (ARPKD)- • bilateral- diffusely enlarged kidneys, • renal failure • maldevelopment of intrahepatic bile ducts • Individual cysts too small to see, distorted kidneys • No cure- renal transplant is necessary • usually bilateral nephrectomy necessary to stabilize cardiac/ lung function with the patient on dialysis until transplant.
Renal Tumors • Renal carcinoma- RCC • Hypernephroma- most common renal neoplasm • >40 with painless hematuria • 10% involve ca++ and tumor necrosis • 90% malignancy in masses with ca++ (nonperipheral) • Triad= hematuria, flank pain, palpable abdominal mass • Radiographic • Bulging or generalized renal enlargement • Infiltration can lead to distortion- obliteration of collecting system or tumor invasion into the vein • US- solid mass, internal echoes and no enhancement • CT- solid neoplasm homogeneous / post injection increased density • Best modality for spread to ipsilateral side/ vein or lymph nodes
Wilm’s tumor- pediatrics • Nephroblastoma • Most common abdominal neoplasm of infancy/ childhood • Arise from embryonic renal tissue • May be bilateral • Highly malignant • Must be differentiated from neuroblastoma • Adrenal -2nd common • US distinguish Wilm’s from hydro • solid appearance • Distortion of renal structure • Demonstrated intrarenal location of mass (neuro- extrarenal) • CT for tumor invasion into renal veins/ IVC or recurrence
Bladder carcinoma • Originates in the epithelium • Urothelial carcinoma- (previous TCC) • Men > 50- 4th most common cancer in men • Cigarette smoke, parasitic infection in Egypt • Radiographic • Finger-like projections into lumen • Polypoid defect arising from bladder wall or focal bladder wall thickening • CT with a full bladder can demonstrate estravesical extension in pelvis- lymph nodes
Renal vein thrombosis • Most frequently in children severely dehydrated • Adult- complication of another renal disease • Glomerulonephritis/ Amyloidosis/ pyelonephritis • trauma • Extension of thrombus from IVC • Direct invasion • Extrinsic pressure from renal tumor • Radiogrpahic • Unilateral/ bilateral • Sudden- causes striking kidney enlargement • Longstanding will become small, atrophic nonfunctioning kidney • Partial or with collaterals- kidney enlarges- collecting system is stretched • US first modality- enlarged kidney with decreased echogenicity from edema- doppler can show the extent of the clot (CT does not) (also no iodine which is hard on the kidneys)
Acute renal failure • Rapid deterioration in kidney function • Accumulation of nitrogen waste in the blood “fishy” • Pre-renal failure- • <blood flow to kidneys from low blood volume- hemorrhage, dehydration, surgical shock, cardiac failure or renal artery obstruction • Post-renal failure- • Obstruction of urine outflow from both kidneys (oliguria) • Prostatic disease, obstruction of bladder neck • Acute renal failure can be from: • Kid disease-glomneph, acute pyelo, severe HTN • Nephrotoxic agents- antibiotics, radiographic contrast, anesthetic agents, heavy metal, organic solvents, hemolysis, >myoglobin • US useful for dilated ureters, renal size, focal lesions, cystic disease- useful so that contrast does not have to further damage the kidney
Chronic renal failure • Reflection of prerenal, postrenal or intrinsic kid disease • Bilatren art stenosis, bilatureteral obstruction, glomneph, pyelo and familial cystic diseases. • Uremia- failure to clear nitrogen waste, accum of urea and creatinine • Toxic effects: nausea, vomiting, diarrhea, drowsiness, dim vision, <mental ability, convulsions, coma • Failure to synthesize erythropoietin- leads to anemia • Pruritus- itching of skin, sallow (yellow) pigment • >water retention due to >sodium- edema and CHF • <serum ca++ - muscle twitching > ca++ from bones- kid stones • Radiographic • US best to eval = small echogenic kidneys • Hydro, renal size, focal lesions, cysts