Download
1 / 10
660 likes | 4k Views
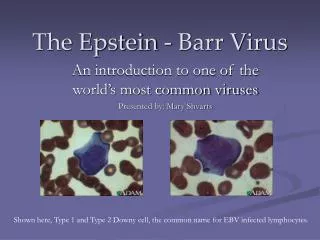
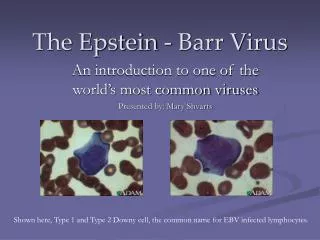
The Epstein - Barr Virus. An introduction to one of the world’s most common viruses Presented by: Mary Shvarts. Shown here, Type 1 and Type 2 Downy cell, the common name for EBV infected lymphocytes. General Information on EBV. Known as EBV, it is one of the best studied viruses.

E N D
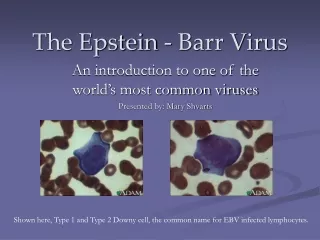
The Epstein - Barr Virus An introduction to one of the world’s most common viruses Presented by: Mary Shvarts Shown here, Type 1 and Type 2 Downy cell, the common name for EBV infected lymphocytes.
General Information on EBV • Known as EBV, it is one of the best studied viruses. • Epstein- Barr may be the most common virus in the world, affecting 80 - 90% of adults worldwide. • A latent, or lysogenic, virus - stops reproducing and remains dormant for period of time before becoming active again. During this latent period, the host has no detectable symptoms, antibodies or virions. • Affects only humans • Targets B- lymphocytes • Linked to diseases such as infectious mononucleosis, Burkitt’s lymphoma, nasopharyngeal carcinoma, and others.
Taxonomical Information Linear, double stranded DNA virus; linear in mature virions, circular in latent form - ex/ lambda phage, adenoviruses • Family of Herpesvirudae – known as Herpes Type 6 • Size - ~120 nm enveloped, 100- 110 nm capsid - Subfamily Gammaherpesvirinae (lymphoprofilerative viruses) - Genera Lymphocryptovirus • Icosahedral capsid symmetry, 162 capsomeres in arrangement • Capsid assembly at nuclear membrane • Nucleic acid replication in nucleus • Budding at nuclear membrane
How does EBV replicate? • EBV enters the cell by attaching to a host cell surface receptor protein (C3d complement protein). • Viral DNA forms into a circle in the host cell’s cytoplasm, enters the cell’s nucleus, and incorporates itself into the cell’s genetic material. • Viral proteins are now expressed. • Ex/ EBNA- 1 – crucial to EBV’s survival within the cell. • The host cell’s immune system recognizes these proteins as foreign and releases T cells to release cytokines in order to destroy the infected host cell. • However, this process is not 100% effective and the EBV virus continues infecting the host for life in a few remaining B- cells in the host’s blood and throat. Image depicting viral attachment and insertion of an EBV virion into a host cell’s genome.
Infectious Mononucleosis • Also known as “glandular fever” and “mono,” this disease is most readily linked to EBV. • Spread through contact with saliva, enters lymphatic tissues and infects B cells. • Infected B cells take on an atypical appearance and are known as Downy cells. • Symptoms include enlargement of lymph nodes and spleen, sore throat, headache, nausea, mild fever, tiredness, and weakness. • Peak occurrence is with the 15-25 year old population. About 50% of college students have no immunity to EBV. About 25-50% of these will contract the disease. • Lower economical classes acquire immunity through early childhood infection. • These infections usually have no symptoms and are undistinguishable from other mild illnesses of childhood. • EBV does not cause problems during pregnancy. • No preventative measures should be taken. • No specific treatment is advised for infection except for treatment of symptoms, which may include a course of steroids to control swelling of the throat and tonsils.
In most cases fever, pharyngitis and swollen lymph glands are used for a clinical diagnosis in determining mono infection. Serologic tests that show an elevated white blood cell count, increased total number of lymphocytes, along with a positive reaction to a “mono spot” test are used as well. If the symptoms of mono are shown, a Paul- Bunnell heterophile antibody test result is needed and no further testing is necessary. IgM immunoglobins to the viral capsid appear early in infection and disappear within 4-6 weeks. IgG’s appear in the acute phase, peak 2-4 weeks after onset, decline and remain for life. Antibodies to the EBNA (EBV nuclear antigen) can be seen by immunoflourescent tests and are only seen 2-4 months after onset. False results are seen often and pseudo-outbreaks have occurred due to laboratory error. Puerto Rico, 1999 How to Determine Infection Mono- Specific Testing EBV- SpecificTesting
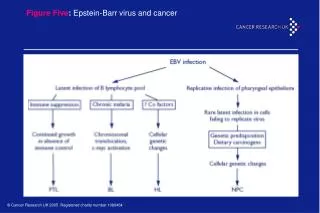
EBV does not cause disease, but its constant gene translocations can. EBV antibodies are produced in excess and if an oncogene happens to be placed next to a gene for antibody production, then oncogenes will also be produced in excess. This results in cancers, such as those seen below. Burkitt’s Lymphoma and other EBV-linked diseases • Nasopharyngeal carcinoma is a tumor of the nasal passages and throat that affects up to 2% of people in southern China. It also occurs in parts of Southeast Asia, northern Africa, and among those living in the Artic. • Has been said to be a possible cause of Hodgkin’s disease. • Oral hairy leukoplakia involves a large amount of replication of EBV in cells around the edge of the tongue, found mostly in AIDS sufferers. • Burkitt’s lymphoma is a non- Hodkins lymphoma which is commonly seen as a malignant tumor of the jaw and abdomen, found mainly in children of central and western Africa. Affects 8 in every 100,000 children in Africa and Papau New Guinea.. • Link to presence of Malaria. Rapid replication of EBV causes mistakes.
History of Epstein- Barr • In 1961 while working as a surgeon in Uganda, Denis Burkitt reported a high incidence of tumors in African children, in certain geological areas. This disease became known as Burkitt’s lymphoma. • Due to the geographical coincidences, researchers M.A. Epstein, Y.M. Barr, and B.G. Achong began looking for cancer- causing viruses from tumor samples sent from Africa. • In 1964, with the help of an electron microscope, they discovered a new member of the herpes viruses now known as the Epstein- Barr virus. Uganda – where the Epstein- Barr virus first was recognized in Burkitt’s lymphoma
New Progressions in the Fight Against Epstein- Barr • Scientists at the Queensland Institute of Medical Research, located in Australia, are working on a vaccine that utilizes a peptide identical to the EBV antigen EBNA-3 to stimulate production of T cells. • This will serve as a vaccine against glandular fever and lymphoproliferative diseases, not EBV. • A 2001 Harvard School of Public Health study shows that there may be a link between EBV and Multiple scleroris. • Blood samples from 62,000 women were tested from 1989 to 1999. Elevated levels of EBNA-2 antibodies were associated with a 4- fold increase in MS. • In a test done by doctors at the Nagasaki University Graduate School of Biomedical Sciences, CD4 T cells obtained during the acute phase of mononucleosis were more readily infected with HIV than were those taken during the convalescent phase. This shows that EBV, like many STD’s, can facilitate HIV transmission and enhance HIV replication. • Social class may have a role in EBV infection with Hodgkin’s patients. To the right – study results of EBV infection vs the Townsend index.
References • Boggs MD, William. “Mononucleosis UPS Risk for HIV Infection.” MEDLINEplus. 25 Nov 2003. National Library of Medicine, National Institute of Health. 06 Dec 2003. http://www.nlm.nih.gov/medlineplus/news/fullstory_14831.html • “Burkitt’s Lymphoma Resources.” Burkitts.org. 10 May 1999. 06 Dec 2003. http://www.burkitts.org/ • “Epstein-Barr Virus and Infectious Mononucleosis.” Centers for Disease Control and Prevention. 26 Oct 2002. National Center for Infectious Diseases. 03 Dec 2003. http://www.cdc.gov/ncidod/diseases/ebv.htm • “High levels of Epstein- Barr Virus Antibodies in Women Linked to Risk of Multiple Sclerosis.” Harvard School of Public Health. 26 Dec 2001. 06 Dec 2003. http://www.hsph.harvard.edu/press/releases/press12262001.html • Hutchins, Andrew.“Epstein- Barr Virus.” UK Disease Directory. 28 Oct 2001. 04 Dec 2003. http://www.diseasedir.org.uk/infect/vir02.htm • “Kissing the Epstein-Barr virus goodbye?” NOVA- Science in the News. Nov 1997. Australian Academy of Sciences. 05 Dec 2003. http://www.science.org.au/nova/026/026key.htm • Prescott, Lansing M., John P. Harley, and Donald A. Klein. Microbiology, Fifth Edition. New York: McGraw- Hill Higher Education, 2002. • “Uganda.” The World Factbook. CIA. 01 Jan 2003. 07 Dec 2003. http://www.cia.gov/cia/publications/factbook/geos/ug.html
![Epstein Barr Virus [EBV] - Named after Epstein and Barr](https://cdn5.slideserve.com/9727845/epstein-barr-virus-ebv-named-after-epstein-dt.jpg)
