Download
1 / 18
180 likes | 339 Views
Complicated Superficial Venous Disease . Ron Bush, MD, FACS Midwest Vein & Laser Center Dayton, OH. Disclosures. Dornier, VeinGogh, VeinExperts.org, BushVenousLectures.com. My Experience.

E N D
Complicated Superficial Venous Disease Ron Bush, MD, FACS Midwest Vein & Laser Center Dayton, OH
Disclosures Dornier, VeinGogh, VeinExperts.org, BushVenousLectures.com
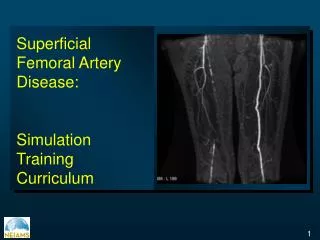
My Experience • In my 17 years of a purely venous practice, the most complicated aspect of superficial disease are the aneurysms of the GSV, AAGSV, & SSV • Most are benign in presentation • Potentially lethal • Inappropriate treatment may make a benign condition be malignant
Definition of Aneurysm Conflicting • Pascarella, 2005, define an aneurysm as 1.5x contiguous vein diameter • (Gabrielli, 2012) – 2.0x contiguous diameter or 3x normal vein size • Only histologic evaluation can differentiate aneurysm from dilatation • But dilatation may mimic same presentation and clinical outcome as an aneurysm
Type II aneurysm • Treated with thermal ablation, stripping, or phelbectomy
SSV Aneurysm • At SPJ junction, excision is the only option • Mimics popliteal aneurysm • Distal aneurysm can be excised, ablated, or foam and depends on the size
Treatment of GSV Aneurysm • Conventional treatment – high ligation • But treatment can be individualized depending on anatomic location • Post-terminal vs. post-subterminal valve • Contradicts Pacarella and Bergan’s report
AAGSV Aneurysm • This should be classified as a Type V aneurysm, since it is a distinct aneurysm • True incidence not known • May be associated with GSV aneurysm • Treatment depends on diameter of connection to GSV connection- ligation • Small connection – thermal ablation of distal trunk or foam
Etiology • Long standing venous hypertension • Turbulent flow at valve • Increased BMI
Final Considerations • Consider unloading GSV circuit before definitive treatment (Personal communication – Allesandro Frullini, MD) • 4-6 months later, there may be substantial reduction in aneurysm size • Treatment can be individualized, but any persistent aneurysmal dilatation post terminal valve including junctional branches should be resected
Final Considerations • All SSV aneurysms involving SPJ are excised • Inappropriate treatment may lead to clot propagation and possible pulmonary embolus
References • Pascarella L, Al-Tuwaijri, Bergan J, & Mekenas L. Lower extremity superficial venous aneurysms. Ann Vasc Surg 2005;19:69-73.