Download
1 / 28
280 likes | 600 Views
Frozen Section of Sentinel lymph node for Ductal Carcinoma in Situ (DCIS). Dr Cheung Chi Ying Genevieve. Cox CE, Ann Surg. 1998. Introduction. SLNBx is well recognized in invasive breast cancer avoid full axillary dissection decrease the morbidity associated with axillary dissection

E N D
Frozen Section ofSentinel lymph node forDuctal Carcinoma in Situ (DCIS) Dr Cheung Chi Ying Genevieve
Cox CE, Ann Surg. 1998 Introduction • SLNBx is well recognized in invasive breast cancer • avoid full axillary dissection • decrease the morbidity associated with axillary dissection • Surgical techniques were well described and were mastered by many surgeons
SLNBx in DCIS • Increasing interest of SLNBx in other applications in breast surgery • DCIS • DCIS is the precursor of invasive cancer
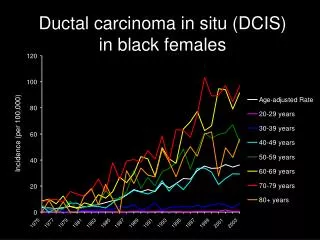
Incidence of DCIS is increasing in the screening era • From 3/100000 to 34/100000 in 50-69 y.o. • Prognosis of pure DCIS is excellent • 5 years survival >95% Van Steenbergen LN et al, breast cancer rest treat. 2009
Controversial issues Pre op trucut biopsy of DCIS not 100% ! About 29.9% of these group had upstaging of disease in final pathology WK Hung et al, Breast cancer 2009
Controversial issues Pure DCIS theoretically will not have any LN metastasis Management of axilla SLNBx for F.S.? Axillary dissection or not? If not -> miss the invasive disease that need AD? Veronesi P et al, Breast. 2005
Current recommendation • Selective application in high risk DCIS • Extensive microcalcifications • Palpable mass • High nuclear grade • Requiring mastectomy • SLNBx is not possible as a 2nd procedure Schneider C et al, Am Surg. 2010 D’Eredita G et al, Tumori. 2009
KWH experience inSLNBx for DCIS • In KWH, SLNBx technique was introduced for DCIS since year 2002 • Results of KWH experience of SLNBx in DCIS are being presented here
Patients • Retrospective study • Period: 3/2002 till 6/2010 • Total number of patients: 170 • Inclusion • Preop trucut Biopsy: DCIS
Patients • Exclusion • Patient with microinvasive disease on trucut bx • Patients with DCIS diagnosed after OT • Mean age: 54.4 years old
Methods of mapping • Methods used for localization of SLN • Blue dye method • Intra-op sub-dermal injection of Patent Blue • Isotope method • Pre-op scintigraphy with 99m Tc Sulfur colloid • Localization with intra-op hand-held gamma probe • Combined
Frozen section The sentinel LN would be sent to the laboratory immediately The pathologist would then give a verbal report Whether the LN is positive for any macrometastasis
Results • SLNBx was successful in 162 (95%) of patients • 5 patients (3%) had +ve SLN on frozen section intraoperatively • Axillary dissection was carried out
Results • 12 patients (7%) had false –ve FS • Axillary dissection was carried out in 6 of them
Pre-op core biopsy : DCIS170 SLN Failed8 (5%) SLN Successful162 (95%) F.S. +ve5 (3%) F.S. –ve157 (92%) False –ve12 (7%) True –ve145 (85%) 3 A.D. –ve(2%)2 A.D. +ve(1%) A.D. 6(3.5%) No A.D.6 (3.5%)
Pre-op core biopsy : DCIS170 SLN Failed8 (5%) SLN Successful162 (95%) F.S. +ve5 (3%) F.S. –ve157 (92%) False –ve12 (7%) True –ve145 (85%) 3 A.D. –ve(2%)2 A.D. +ve(1%) A.D. 6(3.5%) No A.D.6 (3.5%)
Discussion • 11 axillary dissections were done • Only 3 of them were +ve in AD • Final pathology • invasive ductal carcinoma
SLN Successful162 (95%) SLN for P.S. Positive17 (10%) Negative145 (85%) No A.D.6 (4%) A.D. 11 (6%) DCIS3 (2%) Invasive ductal CA8 (5%) All AD -ve AD –ve 5 (3%)AD +ve 3 (2%)
SLN Successful162 (95%) SLN for P.S. Positive17 (10%) Negative145 (85%) No A.D.6 (4%) A.D. 11 (6%) DCIS3 (2%) Invasive ductal CA8 (5%) All AD -ve AD –ve 5 (3%)AD +ve 3 (2%)
SLN Successful162 (95%) SLN for P.S. Positive17 (10%) Negative145 (85%) No A.D.6 (4%) A.D. 11 (6%) DCIS3 (2%) Invasive ductal CA8 (5%) All AD -ve AD –ve 5 (3%)AD +ve 3 (2%)
For pure DCIS with +ve sentinel lymph node either in F.S. or paraffin section SLN is the only LN that is +ve rest of axilla is -ve Discussion
Axillary dissection and intraop frozen section for pure DCIS is unnecessary Discussion
For pure DCIS, taking out the SLN would be enough without the need of further axillary dissection Discussion
Hypothetically, if no F.S. was done for DCIS Potentially save 162 frozen sections 3 axillary dissections Discussion