LYME DISEASE
LYME DISEASE. Lyme Disease. Controversial Suboptimal diagnostic testing Transmitted by Ixodes ticks May also transmit Babesia and Anaplasma Variable disease presentation Cutaneous Cardiac Rheumatologic Neurologic Treatment is longer than for other spirochetal illnesses.

LYME DISEASE
E N D
Presentation Transcript
Lyme Disease • Controversial • Suboptimal diagnostic testing • Transmitted by Ixodes ticks • May also transmit Babesia and Anaplasma • Variable disease presentation • Cutaneous • Cardiac • Rheumatologic • Neurologic • Treatment is longer than for other spirochetal illnesses
Historical Context • 1883 – Buchwald, degenerative skin d/o • 1902 – Herxheimer, ACA • 1909 – Afzelius, EM rash post tick bite described • 1913 – Lipschutz, ECM rash described • 1921 – Afzelius case reports, associates Ixodes ticks • 1930 Hellerstrom, links EM and lymphocytic meningitis • 1941 – Bannwarth, lymphocytic meningoradiculitis • 1946 – Svartz, PCN for ACA
More Historical Context • 1948 – Lenhoff, spirochetes on EM • 1950 – Hellerstrom, ECM with meningitis treated with PCN • 1955 – Binder, 355 cases of ECM treated with PCN • 1968 – Scrimenti, first case of EM in US reported • 1975 – Murray (Lyme resident) reports cases in relatives and friends in area • 1975 – Steere identifies cases as “Lyme arthritis”
Even More Historical Context (?) • 1997 – Steere, defines more complete case description (cardiac, rheum, neuro) • 1980 – Steere, rx with PCN or tetracycline • 1982 – Burgdorfer, discovers spirochetes in blood, CSF, skin lesions of Lyme patients • 1997 – genome sequenced • 1999 – vaccine marketed
Meet the Pathogen • Borrelia burgdorferi has has at least 132 functional genes (c/w about 22 for T pallidum) • Most plasmids of any bacteria identified to date • Antigenic variation/quorum sensing to evade immune response • Dormancy? Cyst structures form in vitro
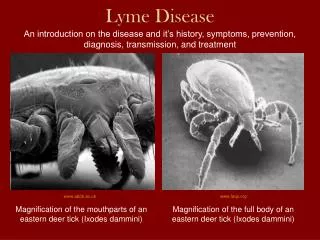
Lyme Disease Vectors • Ixodes scapularis (east and midwest) • Ixodes pacificus (west) Deer / blacklegged tick, Ixodes scapularis Western blacklegged tick (Ixodes pacificus)
From left to right: The deer tick (Ixodes scapularis) adult female, adult male, nymph, and larva on a centimeter scale.
I. scapularis larvae and nymphs feed on the white-footed mouse (Peromyscus leucopus)
I. scapularis adult ticks feed on white-tailed deer (Odocoileus virginianus)
I. pacificus is infected by the dusky-footed woodrat (Neotoma fuscipes), but prefers to feed on lizards, which are not infected
Lyme Disease • Most common tick-borne disease in US and Europe. • Affects 50 nations worldwide • Nymphal ticks are primarily responsible for Lyme transmission to humans. • Tick must feed for ~ 48 hours and become engorged before risk of transmission becomes substantial. • Risk of infection after a deer tick bite in a highly endemic area is ~1.4%.
Lyme Disease Exposure • Obtaining Lyme serology at the time of tick bite is not recommended. • Prophylactic one time use of 200 mg doxy can be considered if: • 20% or more of local ticks are Bb+ (this is generally true in East only) • The patient presents within 72 hours of Ixodes bite • The tick was attached for 36 hours or more. • No contraindication to doxy • Analysis of ticks to determine whether they are infected is not recommended.
Lyme Disease Stages • Early local infection • Skin - EM • CNS • Early disseminated infection • Skin • Multifocal EM • Lymphocytoma cutis (Europe) • Heart • Heart block • Musculoskeletal • Nervous System • Ocular • Conjunctivitis • Late stage infection • Skin • Musculoskeletal • Oligoarticular arthritis • Nervous system • Eye • uveitis
Lyme Disease - Early • EM: • Erythema migrans appears 3-30 (usually 7-10) days after tick bite, commonly on thigh, groin, axilla. • EM recognized in 70% of patients with objective evidence of B. burgdorferi infection. • Early symptoms may include fever, malaise, headache, myalgias, arthralgias, meningismus.
Lyme disease • Erythema migrans • Clinical diagnosis – testing not indicated • Annular or macular • History of tick bite in only 25% of cases • Location: Skin/folds and creases • By definition at least 5 cm in size (controversial) • Lesions may grow 2-3 cm/day • Multiple EM reflective of disseminated disease (hematogenous)
Early Disseminated Lyme Disease • Multiple EM 3-5 weeks after tick bite. • Cranial nerve palsies (especially facial nerve—can be bilateral). • Aseptic meningitis. • Carditis 5% (AV block). • Myalgias, arthralgias, headache, fatigue.
Lyme Disease • Lyme Lymphocytoma • May be associated with EM lesion
Late Lyme Disease • 80% of untreated patients will develop some manifestation of late disease • Arthritis (mono- or oligoarticular, affecting large joints, especially the knee). • Encephalitis/encephalopathy. • Polyradiculopathy.
Lyme: Neurologic • Early local infection (<30 days) • EM with CNS seeding (HA, stiff neck, cognitive difficulties) • Flu like syndrome with CNS seeding • Early disseminated infection (<3 mo) • Aseptic meningitis • Meningoencephalitis (acute cerebellar ataxia, acute myelitis) • Cranial nerve palsy (facial) • Acute painful radiculoneuritis
Lyme: Neurologic • Late persistent infection (>3 mo) • Encephalopathy • Chronic axonal polyradiculoneuropathy • Chronic encephalomyelitis
Lyme: Cardiac • 4-10% of Lyme Disease patients develop carditis • AV block • 40% Wenkebach • 50% complete • Myocardial involvement
Lyme: Arthritis • Emerges in 60% of untreated EM within 6 months average • Intermittent attacks • Asymmetrical • Usually large joints especially the knees • May involve the TMJ
Chronic Lyme Disease • No formal definition: persistent (predominantly neurologic) subjective symptoms that date to initial Lyme disease illness • Most likely heterogeneous and multifactorial causes involved • Persistent infection • Post infectious immune/inflammatory syndrome • Co infection • Reinfection • Fixed deficits • Alternative diagnosis • Hypochondriasis • Most patients do not respond to antibiotics • Medical Clinics of NA 2002;86(2)
Lyme Disease: Diagnosis • Erythema migrans is the only manifestation of Lyme sufficiently diagnostic to be clinically diagnosed without lab testing • Serology (ELISA) • Only 30-40% of patients with EM have a positive serology. • IgM antibodies appear in 3-4 weeks, may persist despite treatment. • IgG antibodies appear in 6-8 weeks, usually remain detectable for many years. • 2-4 weeks after acute reaction 70-80% are positive • Western blot • Indicated for positive or equivocal ELISA. • IgM is only diagnostic within the first month of illness.
Western Blot Up-To-Date 2004
Lyme ELISA • False positive • Other spirochete (syphilis) • Cross reaction with other bacterial heat shock protein (RMSF, Ehrlichia) • RA • SLE • Mononucleosis
Lyme: Diagnosis • IFA: At least as sensitive and specific as the ELISA • Immune assays of CSF • ELISA
Lyme: Diagnosis • Cultivation • Barbour-Stoenner-Kelly (BSK) broth medium • Sensitive for detection of early-phase infection (EM) • Limited value for detection of infection during late stages • Very few places can do this • Skin biopsy or blood taken within first 2-3 weeks of infection
Lyme: Diagnosis • Histology • Numbers of B. burgdorferi in tissues is low • Very hard to find on specimens • Silver stain • PCR • Limited places are able to do this • Urine PCR is available but there is insufficient evidence of its accuracy, predictive value, or its significance • Unclear of benefit of this test
Lyme Disease: Treatment • Early localized • Doxycycline 100 bid or amoxicillin 500 tid or Cefuroxime 500 mg po bid x 14-21 days. • Early disseminated • Isolated facial nerve palsy/mild carditis: doxy/amoxicillin. • Meningitis/severe carditis: ceftriaxone 2gm qd x 14-28 days. • Late disease • Arthritis: doxycycline or amoxicillin or ceftrixaone or IV PCN x 28 days. • Recurrent arthritis: ceftriaxone. • CNS disease: ceftriaxone or IV PCN. • Facial palsy alone: oral meds may be enough
Lyme Disease: Treatment • Cardiac • 1st degree AV block: oral meds • High degree AV block: Ceftriaxone for 14-21 days or IV PCN for 28 days