Download
1 / 64
640 likes | 1.4k Views
Moria One Use- Plus SBK vs. 60 kHz IntraLase FS SBK . Richard J. Duffey, MD**. **sadly, no financial interests. Alternate Title. Do I really need to throw away my microkeratome and buy a femtosecond laser to provide state-of-the-art SBK thin flap LASIK?. ONE Use- Plus SBK

E N D
Moria One Use-Plus SBK vs.60 kHz IntraLase FS SBK Richard J. Duffey, MD** **sadly, no financial interests
Alternate Title • Do I really need to throw away my microkeratome and buy a femtosecond laser to provide state-of-the-art SBK thin flap LASIK?
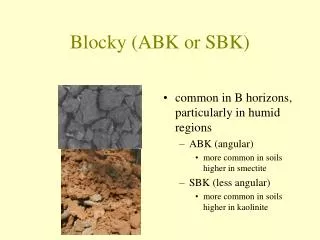
ONE Use-Plus SBK Sub Bowman’s Keratomileusis The Moria option for SBK
Reported advantages of SBK compared to conventional LASIK • Less weakening of corneal biomechanics, less risk of ectasia, better stability • Faster visual recovery • Better quality of vision: • Fewer higher order aberrations • Better contrast sensitivity • Fewer complications, less glare, fewer halos • Less incidence of postoperative dry eye • Reduced loss of corneal sensitivity • Ability to treat more patients, and higher levels of myopia • Can treat thinner corneas • Reduced enhancement rate
The rationale of SBK Anterior third of the stroma is the strongest region of cornea By John Marshall, PhD, UK
The rationale of SBK Less disruption in the anterior third of the stroma causes less weakening of the cornea By John Marshall, PhD, UK
The Moria option for SBK or Sub-Bowman’s Keratomileusis ONE Use-Plus SBK
Demographics • Fifty myopic eyes of 25 consecutive patients • Eleven females, 14 males • MRSE mean: -3.57 +/- 2.17 D (-1.13 to -10.00) • Refractive cylinder mean: 0.53 +/- 0.56 D (zero to +3.00)
Measurement Parameters Preop Intraop • BSCVA • MR and CR • Visx Wavescan HOA • Orbscan II • US Pach • Flap thickness (US pachymetry subtraction method) • Flap diameter • Hinge length (in degrees) • Suction time • Pupil Tracking success • Iris Registration success • Flap status • Stromal bed smoothness • Epithelium status
Measurement Parameters Postop Day 1 Postop Month 1 • UCVA • Flap status • Epithelium status • UCVA • BSCVA • Visx Wavescan HOA • Visante OCT flap profile • Flap status • Epithelium status
Materials and Methods • One surgeon (RJD) using the Moria One Use-Plus SBK automated microkeratome to produce a 100 micron flap • VISX S4 Smooth Scan Active Trak excimer laser with 39 custom ablations and 11 conventional ablations • Follow-up period of one month on all eyes
Results • Flap Thickness: 103 +/- 9 µ (83 to 123) • Vertical Flap Diameter: 9.3 +/- 0.3 mm • Hinge Length: 63° +/- 18° • Pupil Tracking success: 100% • Iris Registration success: 81% • *No epithelial defects or slides • Very smooth and dry beds • No flap striae, microstriae, slipped flaps, free caps, buttonholes, DLK, epithelial ingrowth, etc.
*Why such epithelial kindness? • Disposable smooth heads without imperfections and irregularities from autoclaving, handling, and reusing • Consistent translation speed relative to old manual LSK-One microkeratome
Accuracy and predictability equivalent to Femto-SBK 1. Duffey RJ. One Use-Plus SBK Clinical studies. Presented at Moria’s speaker forum during the annual meeting of American Society of Cataract and Refractive Surgery; April 5, 2008; Chicago, IL, USA. 2. Kerizian G. Will laser microkeratomes replace conventional ones? Paper presented at the ISRS/AAO meeting during the annual meeting of ESCRS in September 2006, London, UK.
Results UCVA @ Day 1 UCVA @ Month 1 • 20/15 38% • 20/20 52% • 20/25 10% • 20/15 50% • 20/20 40% • 20/25 8% • 20/30 2% • MRSE: -0.09 +/- 0.29 D
Visual recoverywith One Use-Plus SBK UCVA at Day 1 postop N=50 eyes
Why Increased UCVA on Day 1? • Thin flaps (this has been my experience with thin flaps for over 5 years, although UCVA has been improved even further with the One Use-Plus SBK) • ? Stretched edges with “whale’s tail” ?
Faster visual recoverywith One Use-Plus SBK UCVA at Day 1 postop One Use-Plus SBK (Dr Duffey): N=50 eyes Intralase 60kHz (Dr Durrie): N=50 eyes
Visual recoverywithOne Use-Plus SBK UCVA at Month 1 postop N=50 eyes
Faster visual recoverywith One Use-Plus SBK UCVA at Month 1 postop One Use-Plus SBK (Dr Duffey): N=50 eyes Intralase 60kHz (Dr Durrie): N=48 eyes
Change in HOA (rms) Results at 1 Month • Total HOA: 0.10µ increase • Coma: 0.04µ increase • SA: 0.08µ increase
Change in HOA between preop and 1 month postop with One Use-Plus SBK and FS 60kHz Blue- One Use-Plus n=50 Yellow- IntraLase FS n=11
Change in High Order Aberrations betweenpreop and 1 monthpostop No clinically significant difference between customized SBK treatment using IntraLase 60kHz & One Use-Plus SBK; both better than PRK data.
Visante OCT (2.01) Flap Profile Results at 1 Month • Planar and near planar flap profiles that match photos from published IntraLase studies (Stahl, Durrie, et al.) and compare equally between One Use-Plus SBK and IntraLase FS 60 kHz SBK in this study. • ***As with all OCT profiles (even with the latest 2.01 software), it is impossible to consistently identify the interface and accurately place the cursor on it at the 1 month postop visit, thus decreasing the reliability of central, paracentral, and peripheral flap thickness measurements…both in the OUP and FS laser cut flaps. • ***Very subjective endpoints for flap thickness measurements with the present state of OCT technology
AAO 2007: Predictability of flapthicknesswith -1 disposable ring of One Use-Plus • James Lewis, MD (OCT Visante®) • Zeiss OCT Visante® • 100 +/- 9,6 (83-125) • N = 84 eyes
High resolutioncorneal scans…512 A-scans per line…0.25 sec per line. Four lines total at 45, 90, 135, and 180 degrees…all in 1 sec.
Color One Use-Plus SBK disposable -1 ringflapwith a planar profile at 1 mo.
Color One Use-Plus SBK disposable -1 ringflapwith a planar profile digitized
Grayscale One Use-Plus SBK disposable ringflapwith a planar profile and taper edge
ColorFemtosecond SBK at 1 monthflapwith a planar profile and edgescar
ColorFemtosecond SBK digitizedflapwithplanar profile and edgescar
GrayscaleFemtosecond SBK flapwithdigitizedplanar profile and edgescar
Totallymasked placement of cursors on OU-P flapat 1 monthpostop…not reproducible!!
Totallymasked placement of cursors on FS flapat 1 monthpostop…not reproducible!!
OCT of Flap Interfaces • At present with the best technology available, this is a qualitative test only that helps assess the planar nature of flaps. • It is not sensitive enough nor high resolution enough to be able to reproducibly assess flap thickness quantitatively in all meridia or even along one complete meridian.
Top: Moria OU-P -at 1 month- Bottom: FS 60kH This is the best we can do…a qualitative comparison of the planar nature of both the One Use-Plus and femtosecond laser flaps.
Why Planar Flaps? • ? Meniscus shapes are nullified as the microkeratome flaps become thinner ? …or meniscus shape flaps from longitudinal translational mechanical microkeratomes were a myth to begin with
Moria manual LSK-One 180 micron flap after H-LASIK with slow translation…it’s planar!
Moria One Use-Plus SBK vs.60 kHz IntraLase FS SBK SEM Smoothness Study of the Stromal Beds
Materials and Methods • Four cadaveric eyes (2 paired sets) unsuitable for corneal transplantation • Less than 5 days post mortem
Methods Moria One Use-Plus SBK Femtosecond 60 kHz SBK • One eye from each pair, thus 2 eyes total • 100 micron flap, 9 mm diam., 60° hinge, 7 mm/sec automat. translation, 15,000 oscill/min. • Flap lift and amputate • Cornea removed and placed in gluteraldehyde • SEM prep, scans at 20x, 40x, 80x, and 100x • One eye from each pair, thus 2 eyes total • 100 micron flap, 9 mm diam., 55° hinge angle, raster pattern energy of 1.0 µj, pulse separation 8x8 µm, side energy cut 1.0 µj at 70°, “pocket” enabled • Flap lift and amputate • Cornea removed and… • SEM prep, scans at 20x…
Method of Smoothness Scoring • 10 masked (to technology) observers rated each stromal bed photograph for smoothness on a scale from zero to four (zero was “polished glass smooth”) • Photos were evaluated sequentially by magnification: all 20x photos first, followed by all 40x, followed by all 80x, followed by all 160x photographs • 3 representative photos (chosen by SEM technician) of each of the 4 different magnifications were evaluated for each of the 2 technologies making a total of 12 Moria and 12 femtosecond laser bed photographs that were scored • A cumulative mean score was tabulated for each of the two technologies by combining the 20x, 40x, 80x, and 160x data scores lumped together
SEM: 20x OU-P IntraLase FS
SEM 40x UO-P IntraLase FS
SEM 80x UO-P IntraLase FS
Representative Scoring Scale at 160x: 0 glass…1…2…3…4 1 2 3 4
Edges IntraLase FS 20x OU-P 80x
Scored Results (Mean) Moria One Use-Plus SBK 60 kHz IntraLase FS 2.24 3.78
Scanning Electron Microscopy Moria One Use-Plus vs. IntraLase FS 160x OU-P FS 60kH
Why the difference? • The raster pattern of the femtosecond laser produces a “velcro” like interface that has to be peeled open with increased force to break the remaining adhesions between the pixel pattern bursts of laser energy.