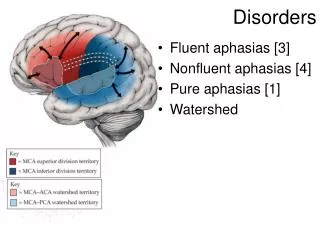
Pubertal disorders
Pubertal disorders. Dr Olcay Evliyaoğlu Pediatric Endocrinology Department. Puberty. Sexual differentiation begins on 4-5th week of gestational age. ADOLE SENCE. Foliküler faz. Phy s ical, sexual, physcological development. Transition to adulthood from childhood Not an adult nor child

Pubertal disorders
E N D
Presentation Transcript
Pubertal disorders Dr Olcay Evliyaoğlu Pediatric Endocrinology Department
Puberty Sexual differentiation begins on 4-5th week of gestational age.
ADOLESENCE Foliküler faz • Physical, sexual, physcological development. Transition to adulthood from childhood • Not an adult nor child • Time of transition • Establishment of individualism.
PUBERTY • Secondary sex characteristics are developed • Includes • Physical growth • Sexual development • Psychological development
Growth spurt, disturbution of muscle and fat • bone maturation and fusion of epiphysical centers • Adult height • At the end of this periodspermatogenesis in boys, ovulation in girls occur
hypothalamus LHRH neurons LHRH Pituitary Gonadotroph cells FSH , LH GONADs Testes Ovaries Testosteron Estradiol HPG axis
STRESS What makes HHG axis work - + + MATURATİON NUTRİTİON CENTRAL NERVOUS SYSTEM LEPTIN GLUTAMAT GABA ENDROFIN + + - - + HYPOTHALAMUS - - GnRH - - - + + PİTUİTARY PRL - - - - LH FSH - - + + OVARY TEKA GRANULOZA ESTROGEN INHIBIN ANDROGEN
Genetic and environmental conditions effect timing of puberty · Environmental factors: • Socioeconomic factors • Nutrition • General health • Geographical place lived
Hypothalamus GnRH pulse frequency and amplitude increase Pituitary LH pulse frequency and amplitude increase At early stages at nights With progression of puberty pulses occur during day
Gonadotropins • FSH, LH • Glucoprotein • Alpha ve beta subunits ( alpha subunits are same, differences are on beta subunits)
FSH • sertoli cells (testis) • Granulosa cells (over) • Stimulate LH rec production on Leyding cells gamotogenesis
LH • Leydıng cells ( testis) • Teca cells ( over) Gonadal steroids
LH Teca cells androstenedion Granulosa cells FSH estrogen
Leydig cells LH testosteron
Adrenarche • Increase in the secretion of adrenal androgens • Appearance of pubic hair (pubarche) • Axillary hair
Adrenarche CRH Hypothalamus Pituitary ACTH Adrenal cortex Adrenal androgens
Nutrition and puberty • Menarche is earlier in obese girls • Malnutrition , chronic diseases, and excessive physical activity delay pubertyand menarche
Timing of puberty is related to bone age rather than chronological age • BA< CY ------------- delay in puberty • BA = CA ------------- puberty on expected age • BA>CA --------------early puberty (puberty precocous)
·girls the first sign of puberty is telarche, generally observed on 10 - 11ages, menarche is observed 2-3 years after telarche. • In girls growth spurt occurs 2 years earlier than boys. Growth spurt in girls is at the time of telarche, • In boys growth spurt occur at the time when testes volumes are 10 ml. • Telarche Pubarche Menarche
Tanner stage 4 2-3years after telarche Menarche
Pituitary hormones Ovarian hormones ovulation corpus albicans follicule corpus luteum ovary İstihdam dominant Seçim istihdam Endometrium Follicular /proliferative phase Luteal /secretuary phase
·In boys initial finding of puberty is enlargement of testes. This is followed by scrotum pigementation and thinning of scrotal skin. Penis enlarges. Pubic hair develops. Growth spurt occurs at 14-16 years and usually continues until 18 years.
PUBERTAL PROBLEMS • Precocious puberty • Delayed puberty • Pubertal gynecomastia • Gynecological problems • Pyschological problems • Sexual identity problems • Eating disorders: Anoreksia nervoza, Bulimia Nervoza • Enuresis Nocturna • Orthopedical problems
PRECOCİOUS PUBERTY • Breast development before 8 years in girls and testes development more than 4 ml or any other pubertal sign before 9 years in boys are considered precocious . • Central Precocious Puberty (CPP):Activation of hypothalamus-pituitary-gondal (HHG) axis. • Peripheric Precocious Puberty (PPP) : Signs of puberty with out activation of HHC axis. Izosexual perifpheric PP: Secondary sexual characteristics are appropriate for the sex of the child. heterosexual peripheric PP: Secondary sexual characteristics are inappropriate for the sex of the child.
Etiology : • Central PP • Idiopathic: sporadik, familial • CNN disorders: Tumors (Optic glioma, hypothalamic gliom, astrositoma, epandimoma, kraniopharengioma), sarkoidosis, suprasellar cysts • Nörofibromatosis, Tuberosclerosis • Peripheric PP • Gonadotropin secreting tumors: Hepatomas, hepatoblastoma, teratoma, choriocarsinoma, germinoma • Any disorder resulting in gonadal steroid secretion Excess androgen: Congenital Adrenal Hyperplasia, testes tumors Excess estrogen: Ovarian cysts or tumors • Mc Cune Albright Syndrome • Activation mutation in LH receptors • Severe hypothyroidism
Central PP: diagnostic criteria • Clinical • Height • Midparental height and target height • Height velocity • Pubertal stage • Bone age
Central PP: diagnostic criteria • Pelvic USG findings supporting CPP • Uterus long diameter 34-50mm • Pear shaped uterus (F/C>2:1) • Endometrial echo specifity (100%) but sensivity (42%-87%) • Ovarian volume <2-3 ml (v:a x b x c x 0,5233) • Follikul number>6 size>8mm
Central PP: diagnostic criteria • Laboratory : 1) Pubertal levels of LH amplitude and pulsity 2) Gn-RH stimulation test: Pubertal LH response peak > 5 IU /L 3) Gn-RH stim LH/FSH>1
Criteria suggesting progressive precocious puberty • Progression of breast staging in less than 3-6 months • Growth velocity > 6cm /year • Bone age advanced more than 1,5-2 years • PAH below target height and decline in PAH during follow up. • Uterine volume>2 ml, long diameter >35 m, endometrial echo • Ovarian volume >2-3 ml • Peak LH>5 mIU/L at GnRH test • Basal LH >0,3
McCune Albright Syndrome • ·Cafe au lait patches on skin • · Polyostotic fibrous dysplasia • ·Endocrine disorders: Peripheric PP Cushing syndrome, hyperthyroidism
Mc cune albrigt - 4.5 years old -polyostotik fibrous dysplasia
Treatment • Goals: • Synchronosing puberty with peers (ameliorating pshchological stress) • Decreasing the rate of bone maturation so as to acheive a normal final height
Treatment(SPP) GnRH analogs. Lucrin 3.75mg IM /month 7,5mg IM /month 22,5mg /3 months 11,25mg months
When to stop treatment • Much depends on the primary goal of treatment , patient – parent preference • Average age of treatment discontinuation • CA:10,6 -11,6 years • BA:12,1 – 13,9 years • Max adult height CA:11-11,5 ve BA: 12-12,5 years
Treatment (PPP) Boys • Antiandrogens ( andr rec inhibition) • İnhibitors of 17,20 liyase ve testosteron synthesis • Aromataseinhibition (arimidex) Girls • Aromatase inhibitors • E2 rec inhibition
İNCOMPLETE PP • Only one pubertal sign. • Premature telarche • Premature adrenarche • Premature menarche
Premature Telarche • End organ increased sensivity • There can be difference in 2 breasts, one can start development 6 months earlier than the other
Premature telarche PP ------------------------------------------------------------------ Growth velocity not increased increased Bone age not advanced advanced Vagen mucosa not obvious obvious E2 effect Uterus size Prepubertal Pubertal GnRH response Prepubertal Pubertal Adrenarche no can be
Premature Adrenarche PP Penis size Prepubertal Pubertal Growth velocity not rapid rapid Bone age not advanced advanced Testes size Prepubertal Pubertal Serum Testesteron Prepubertal Pubertal DHEA-SO4 Prepubertal Pubertal or 17-OH progesterone Prepubertal high in CAH 11-Deoksikortisol Prepubertal high in 11-OH lase deficiency Bazal LH/FSH Prepubertal Pubertal
Puberty tarda-PT (Pubertal delay) • Not if any sign of puberty has been observed in 13 years old girls and 14 years old boys
Males If • Sexual development has not been developed until13.7 years. • Transition from stage II to III is more than 2.2 years • Transition from stage III to IV is more than1.6 years • Transition from stage IV to V is more than 1.9 years • Sexual development has not reached stage V until 17.1 years • Bone age>12 years and pubertal development has not begun
Females If • Breast development not started until 13.4 years • Transition from stage II to III is more than 1 year • Transition from stage III to IV is more than 2.2 years • Transition from stage IV to V is more than 1.8 years • Not menarche at the 5th year of telarche • Bone age >11 and pubertal development has not begun
Etiology of PT • Konstitutional growth and pubertal delay • Hypogonadotropic hypogonadism • CNS disorders: Tumors, congenita disorders, radiation • Isolated gonadotropin deficiency: • Multiple pituitary hormone deficiency • Prader-Willi syndrome • Laurence-Moon, Bardet Biedle syndrome • Chronic diseases • Sudden weight loss, anoreksia nervoza • Hypothyroidism • İncrease in physical activity
Etiology of PT • Hypergonadotropic hypogonadism • Males • Kleinfelter syndrome • Primary testicular insufficiency • Anorchia or kriptorchidism • Females • Primary ovarian insufficiency • Noonan syndrome, Ulrich syndrome) • XX veya XY gonadal dysgenesis • Turner Syndrome
Constitutional growth and pubertal delay • Pubertal development is delayed concordant with growth • CA>BA=HA • Growth velocity is normal • Height sds is between -2sd and -3sd • With the onset of puberty and pubertal growth spurt final height becomes appriate to target height
Treatment (constitutional growth and pubertal delay) 1. Phsychologic treatment 2. Gonadal steroids: 13 years old girls and 14 years old boys who have not developed any pubertal sign can be treated Girls : For 3 months ConjugatedE2 (0.3 mg/day) or ethynyllestradiol (5-10 g /day) Boys : For 3 months testesteron enanthate (50-100 mg/ month) IM Development of pubertal signs and an increase in growth velocity is what expected from this treatment.
Hypogonadism / treatment • Males • By gradually increasing testosterone dose adult dose of 300mg/month is acheived. • In the case of hypogonadotropik hypogonadism to increase endogenous testosterone production and testes size HCG treatment can be initiated • Females • 5 g/ day10 - 20g/ day etynyllestradiol • 0.3 - 0.625 mg/day conjugated estrogen . • With the appearence of physical effects of E2 Medroksiprogesterone acetate on days 12. - 21. of cycle can be added
Gynecomastia • Observed in 30 - 35 % of males • Generally bilateral • In P3 and P4 stages; 14 - 14.5 years • Glandular tissue diameter is generally less than 4 cm, resembles stage II in girls • Glandular tissue > 5cc and resembles stage III and IV in girls Pubertal Macrogynecomastia , do not regress spontaneously
Etiology for pathologic gynecomastia : • Endocrinopathies • Tumors • Chronic diseases • Drugs : Hormones, antidepresants, anti Tbc drugs, etc