Download
1 / 51
610 likes | 840 Views
Strengths focused Treatment. Dr Karen Richard And Dr Lisa Cameron 2013. plus ça change, plus c'est la même chose. Pioneers of strength-focused approach. Local hero William A F Browne. Dr Kirk!!. Assessing protective factors The SAPROF.

E N D
Strengths focused Treatment Dr Karen Richard And Dr Lisa Cameron 2013
Assessing protective factorsThe SAPROF Michiel de Vries Robbé & Vivienne de Vogel Van der Hoeven Kliniek SAPROF Workshop April 2012
What is risk assessment? The assessment of the risk of future (sexual) violent behavior in patients / offenders with a violent history and/or mental disorder
What is violent behavior? Violence is actual, attempted, or threatened harm to one or more persons Webster, Douglas, Eaves & Hart (1997)
3 methods of risk assessment 1. Unstructured Clinical method Based on the experience, training and knowledge of psychiatrist, nurse, psychologist or clinician. 2. Actuarial method Based on empirically found risk factors for violence, standardized, mostly static factors, designed to predict 3. Structured Professional Judgment (SPJ) method Integration 1 & 2: Standardized risk assessment, based on empirically found risk factors for violence and clinical experience.
Structured Professional Judgment • Bridging the gap between science and practice • To be coded by a trained and experienced clinician • Process of coding structures and professionalizes clinical judgment • Not just adding the scores, but interpretation / weighing / combining / discussing items • Repeated assessment is necessary • Assessment leads to consider violence scenarios and planning of risk management
Violence risk assessment Advances Increased knowledge on risk factors for (sexual) violence Major advances in structured risk assessment procedures Shortcomings Almost no information on factors that can compensate for or diminish effects of risk factors Most structured risk assessment instruments do not include protective factors.
Importance of considering protective factors More balance in risk assessment: complete view of the offender Positive approach motivating for both offenders and treatment staff Suggestions for improved risk management Rogers (2000): ‘Risk-only evaluations are inherently inaccurate’.
COMMENTARYThe Uncritical Acceptance of Risk Assessment in Forensic Practice Forensic psychologists are frequently asked to conduct evaluations of risk assessment. While risk assessment has considerable merit, recent applications to forensic psychology raise concerns about whether these evaluations are thorough and balanced. Forensic adult risk-assessment models stress risk factors, and deemphasize or disregard entirely the other side of the equation: protective factors. Mediating and moderating effects must also be considered. Moreover, base-rate estimates may produce erroneous results if applied imprudently to forensic samples without regard to their unstable prevalence rates or the far-reaching effects of settings, referral questions, and evaluation procedures.
Positive / strengths-based approach Good Lives Model (GLM-C) (e.g.Ward et al, 2007) Focus on strengths, therapeutic alliance, holistic, tailored therapy, establishment of skills and competence needed to achieve a better life
Positive / strengths-based approach Desistance (e.g. Maruna, 2001) DESISTANCE AND DEVELOPMENT: THE PSYCHOSOCIAL PROCESS OF 'GOING STRAIGHT' Desistance is seen as a maintenance process, a long term abstinence from crime among individuals who had previously engaged in persistent patterns of criminal offending (e.g. through aging, maturation, “a steady job and the love of a good woman”)
Protective factors background Are protective factors not merely the opposite of risk factors? In general the approach is very different: What strengths are there to build upon What positive goals can be worked towards What can be built up instead of what should be broken down Some protective factors can be risk factors when not present (e.g. Self-control) Some protective factors are generally not risk factors when not present (e.g. Leisure activities; Intimate relationship) How do protective factors influence future violence risk? Remains largely unknown for now, likely: Promotive effect for some factors (work for everybody) Protective effect for other factors (only moderating when risk present)
What are protective factors? SAPROF Any characteristic of a person, his / her environment or situation, which reduces risk of future (sexual) violence De Vogel, De Ruiter, Bouman, & De Vries Robbé (2009)
Risk & Protection Risk factors Risk factors Protective factors Protective factors
We all need protective factors The more it rains (risk factors) the more protection we need
Development of the SAPROF Structured Assessment of PROtective Factors for violence riskDe Vogel, De Ruiter, Bouman, & De Vries Robbé (2007)
Van der Hoeven KliniekUtrecht, The Netherlands Forensic psychiatric hospital: 286 beds Mostly TBS order: involuntary treatment 50/50 personality / psychotic disorders Holistic approach, emphasis on CBT & relapse prevention Therapeutic community: taking responsibility Rehabilitation: gradual through ‘transmural phase’ Risk assessment in consensus HCR-20 & SAPROF (+SVR-20, FAM) Repeated regularly to inform treatment
Sociotherapist Consensus Treatment supervisor Researcher Consensus model • HCR-20 • SAPROF • SVR-20 if sexual offense • FAM if female
Risk assessment at theVan der Hoeven Kliniek 2001: Implementation HCR-20 & SVR-20 Consensus model 2005: Risk assessment mandatory in the Netherlands 2007: Implementation SAPROF 2009: Implementation START specific short-term groups 2011: Implementation FAM Female Additional Manual 2001-2005: Dissertation De Vogel: Dutch HCR-20 & SVR-20 are valid and valuable for forensic practice 2007-2012 Dissertation De Vries Robbé: psychometric properties and value of the SAPROF for forensic practice
Preface of the SAPROF Mental health professionals desired more knowledge on protective factors Research into protective factors is scarce No suitable instruments for medium term prediction of violence for adults
Development SAPROFPreconditions Scientific basis Practically applicable: Dynamic factors, concrete guidelines for treatment, easy to code In line with other risk assessment tools: SPJ model, basis and method similar to HCR-20 / SVR-20; aim = positive addition to these checklists
Additional value of the SAPROF Risk assessment Balance risks and strengths Increased predictive validity violent recidivism and violent incidents during treatment Clinical practice Positive approach Dynamic Improved risk management focus Risk defined in changeable positive factors
SAPROF Versions Dutch English German Spanish Russian SAPROF-YV Italian French English 2nd Norwegian Danish Swedish Chinese Portuguese Dutch 2nd • Dutch version published in 2007: • Implemented in 2007 in the Netherlands • PhD project validation of the SAPROF • English in 2009 • Followed by: German, Italian, Spanish, French, Swedish, Norwegian, Portuguese, Russian & English 2nd Edition • In preparation: Dutch 2nd Edition, Chinese, Danish & Youth version
The SAPROF 17 protective factors (15 dynamic, past 6 months) Three scales: Internal factors Motivational factors External factors Should always be coded in combination with SPJ risk assessment instrument +
Internal factors (static) 1. Intelligence • Level of intelligence (test results) • Recent testing (max 6 years ago) 2. Secure attachment in childhood • Attachment with prosocial adult • Based on file information before the age of 18 • Secure attachment + good example
Internal factors (dynamic) 3. Empathy • Empathy towards others (past/potential victims) • Observation of behavior and emotions 4. Coping • Effective problem solving and conflict management skills • Observation of behavior in daily life + self-rapport 5. Self-control • Impulse control and self restraining in times of stress or temptation • Self-control and perseverance in self-discipline
Motivational factors 6. Work Stable and suitable work Daily structure and personal development Paid/unpaid 7. Leisure activities Structured Prosocial contacts, social control Daily structure and hobby 8. Financial management • Steady income (work or benefits) • Sound financial management, no debts • Sufficient finances for living circumstances Work / Leisure activities not always protective …
Motivational factors 9. Motivation for treatment • Insight in necessity, motivation for change • Openness, cooperation and progress in treatment 10. Attitudes towards authority • Positive attitude, tolerance of authority • Commitment to agreements and compliance with rules and regulations 11. Life goals • Factors that provide meaning and positive life fulfillment (extra motivation to do better) • Religion, parenting, ambitions 12. Medication • Motivation for and compliance with medication • Effectiveness of medication
External factors 13. Social network • Prosocial and supportive • Experienced support of family and friends 14. Intimate relationship • Duration and stability • Quality • Information from partner
External factors 15. Professional care • Availability mental health care • Intensity: frequency and nature of support 16. Living circumstances • Supervision by health care professionals • Social control from related others 17. External control • Mandatory treatment or probation contact • Judicial proceeding • Intensity of mandatory external control
Theory of changing protection Static protective factors 1. Intelligence 2. Secure attachment in childhood Dynamic decreasing factors 15. Professional care 16. Living circumstances 17. External control Dynamic improving factors 3. Empathy 4. Coping 5. Self-control 6. Work 7. Leisure activities 8. Financial management 9. Motivation for treatment 10. Attitudes towards authority 11. Life goals 12. Medication 13. Social network 14. Intimate relationship
Blair Ghost Project Ghosts, Gothic Terror and a bit of Shakespeare… The Blair Ghost Project was a collection of connected scenes devised and performed by patients from the Tayside Area Forensic Service.It was performed at Horsecross Theatre in Perth in 2008 both for invited audience in June and as part of Welcome to the 2nd annual Scottish Mental Health Arts and Film Festival.
The dust never settles… If you could reinvent yourself into anything you wanted, what would it be? The Dust Never Settles is about journeys in the imagination from a Spaghetti Western to dreams of comedy stardom to a late night piano bar. Devised and performed by patients from the Forensic Psychiatry Unit, the piece involves drama, live music, songs and images. Be prepared for some funny moments and some thoughtful moment. Be prepared for change.
Clinicians involved in developing the SAPROF Generated ideas for SAPROF Participated in pilot-study Ongoing feedback on SAPROF in daily practice SAPROF is helpful in: Justifying stages of treatment (leave/privileges, risk management)’ Formulating treatment goals (from external to motivational and internal)’ Phasing treatment: what to do first?’ Clinical experiences with the SAPROF Van den Broek & De Vries Robbé (2008)
“The whole is greater than the sum of its parts.”― Aristotle
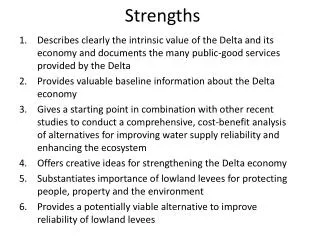
Overview SAPROF • Structured assessment of protective factors • Dynamic and positive addition to risk assessment • Good results research • Especially valuable for clinical practice • Increasingly personalized risk assessment • Positive treatment goals • Strengths based guidelines treatment planning and risk management