Download
1 / 16
160 likes | 213 Views
Learn about Treponema, a genus of spirochaetes, its characteristics, pathogenicity, and associated diseases like syphilis. Explore the stages, diagnosis, and treatment options for this important pathogen.

E N D
COURSE: MICR4002 SPIROCHAETES: TREPONEMA
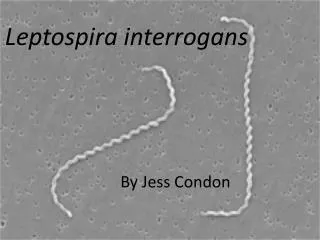
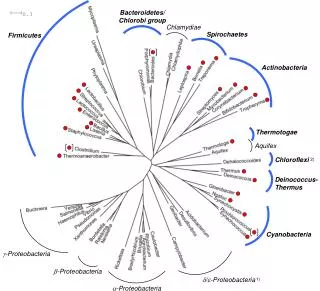
Introduction Spirochaetes are bacteria belonging to the family of Spirochaetacea. They are long, motile and twisted spirally round a long axis. They are found in water, soil and decaying organic matter. They divide by transverse fission and there is no definite nucleus. Many of them are saprophytes and commensals. Genera of Spirochaetes of medical importance are: Treponema Borrelia Leptospira
GENUS TREPONEMA Characteristics: Treponemes are small, slender, flexible cork-screw shaped anaerobic organisms, measuring 5-15um x 0.2um with 6-12 evenly sized coils. They have a slow bending and rotating motility. They cannot be stained by Gram’s stain but can be demonstrated by silver and T. cunicola. But T. pallidum is now classified as T. pallidumsubspecies pallidum and T. pertenue as T. pallidumsubspecies pertenue impregnation method. They are not culturable. Type species: T. pallidum. Other important members of the genus are T. pertenue, T. carateum.
Pathogenicity: T. pallidum subsp. pallidum causes syphilis which is acquired sexually and congenitally. Sexually transmitted syphilis: This STD occurs in 3 stages:
1.Primary syphilis: Onset: 2 – 4 weeks after infection Presentation: Ulcer on the genitalia. Ulcer known as hard chanre – firm, clean and circumscribed. Chancre fluid is rich in treponemes. Ulcer heals up spontaneously in 10 – 40 days. 2. Secondary syphilis: Onset: 2 – 8 weeks after primary syphilis. Presentation: Skin eruptions, red rashes with papules. Widespread multiplication and dissemination in blood. Patient highly infectious. Other symptoms include fever, malaise and general lymphadenapathy. May last from 10 days to 1 year.
3. Tertiary syphilis (early and late latent stages): Early latent stage: This is inactive stage following secondary syphilis. Patient is non-infectious, though feotus of an infected mother can be infected. Late latent stage: Onset is approximately 3 years after secondary stage. Presentation: Inflammatory lesions in any organ or tissue but CNS and cardiovascular systems are mostly involved. Complications may include gummas or granuloma of skin or bone, liver damage, eye impairment and ear dysfunction. Patient is non-infectious except to the foetus of an infected mother
Congenital syphilis: Infected mother transplacentally transmits the disease to the foetus. Congenital syphilis may result in still birth in about 40% of cases and abortion is also frequent. Onset: Signs appear about one year after birth – skin rashes, jaundice, painful limbs, anaemia and saddle-nose. Non-venereal syphilis: This is usually acquired as occupational hazard by doctors, nurses and laboratory workers; or through blood transfusion. The organism gains entry into the body through abraded skin.
Other treponemal infections: T. pallidum subsp. pertenue causes yaws – an endemic disease of tropical countries which is pathologically similar to syphilis but differs in its contagious and non-venereal nature. it produces ulcerating papules on the skin. T. carateum causes pinta – an endemic disease in Mexico, South America and Phillippines. T. cunicola causes rabbit syphilis and morphologically resembles T. pallidum.
Laboratory diagnosis: Specimen: Serous fluid from lesion DG microscopy: Three consecutive specimens must be examined before reporting negative. Culture: This is not done though Reiter’s strain is cultivable. Nichol’s strain is maintained in an adult rabbit testis by serial passaging.
Serology: Syphilis is diagnosed serologically using non-specific screening tests such as RPR and VDRL tests and specific confirmatory tests such as FTA and TPHA tests. The screening tests detect reagin antibody using cardiolipin antigens. The specific tests detect treponemal antibody using treponemal antigens. The routine serological tests are therefore divided into non-treponemal and treponemal tests: Non-treponemal tests: ( non-specific tests): These tests detect reagin antibody, a non specific antibody that is present in syphilitic serum. It appears in a patient’s serum in 10-14 days after exposure. The antigen is cardiolipin antigen which contains alcoholic extract of ox heat muscle to which cholesterol and lecithin are added .These tests are used to :
Screen for active syphilis • As tests of cure • As an aid in diagnosing congenital syphilis. • Non- treponemal tests include the Rapid plasma regain (RPR) test, Venereal diseases reference laboratory (VDRL) test, Unheated serum regain (USR) test etc. They all use the same antigen and easy to perform but RPR and VDRL are the most commonly used. • RPR test is performed on a card and the antigen is coated with charcoal: 50ul of the plasma ( serum or blood ) and a drop of the antigen are mixed on the test card, shaken at 100 rpm for 8 minutes. Agglutination is visible to the naked eye.
VDRL test is performed on a perspex slide and viewed under the microscope. The antigen is not coated and the serum is inactivated at 560C for 30 minutes before the test is done. It is recommended for use with CSF in neurosyphilis. • False positive result is fairly common. This may be due to: • Technical error • Cross reaction with other treponemal species • Biological false positives (BFP): These are due not to technical error but as a result of certain infectious and non infectious conditions such as malaria, mumps, hepatitis, rheumatoid arthritis, tissue damage etc.
Treponeaml test(aka Specific tests): These are tests that detect antibody to T. pallidum subsp. pallidum and other species. These tests are: Treponema pallidum immobilization (TPI) test: The test uses live treponemes which when mixed with the patient’s serum, the antibody in the serum immobilizes the organisms when examined under the darkground microscope.. The treponemes are Nicholl’s strains recovered from the testis of rabbit. The disadvantage is that there is always the risk of infection to the worker, and the method is cumbersome and expensive.
Flourescent treponemal antibody-sorbent (FTA-ABS) test: The test uses Nicholl’s strain as antigen fixed on a slide. Diluted patient’s serum is added on to the antigen, excess washed off and the smear treated with anti human immunoglobulin conjugate. After incubating and washing, the slide is examined under the fluorescent microscope. The test is most specific and sensitive though expensive. It is positive for life.
Treponema pallidum haemagglutination (TPHA): This test is similar to the FTA in sensitivity. Antigen is Nicholl’s strain coated with tanned turkey or chicken or sheep red blood cells ( sensitised cells). A non sensitized cell suspension is used as control. In the presence of treponemal antibody, the treponemes adhere to the sensitized red cells and settle at the bottom of the micro titre plate well as orange to red layer. It is easy to perform, fast and cheap. It is positive for life. • FTA-ABS and TPHA tests are also positive for T. pertenue and T carateum.
DNA probes e.g. (PCR): These are new diagnostic tools that are highly specific and sensitive. As of now, they are very expensive and are not be used routinely.