Download
1 / 34
600 likes | 3.28k Views
Semen analysis & Sperm processing. Jalal Ghasemzadeh. Andrology lab. What is Andrology?. Andrology is the study of male fertility and laboratory aspects of infertility diagnosis and treatments. Science of diseases of males, including infertility, spermatogenesis and sexual dysfunction.

E N D
Semen analysis & Sperm processing Jalal Ghasemzadeh Andrology lab
What is Andrology? Andrology is the study of male fertility and laboratory aspects of infertility diagnosis and treatments. Science of diseases of males, including infertility, spermatogenesis and sexual dysfunction. “Andro” from the Greek “andros”, man.
Semen analysis • Semen analysis (SA) is a gateway test and primary test for evaluation of male infertility and treatment planning for helping couples achieve pregnancy. • Safe, inexpensive, non-invasive procedure • Alternative names : sperm count sperm test male infertility test spermogeram
Indications of semen analysis 1)Assessment of fertility (2 sample,7days to 3weeks) Phosphatase acid 2) Forensic purposes PSA Sperm 3) Suitability for artificial insemination (IUI, IVF) 4) Post vasectomy (2 sample, 3 months and 6 months )
Seminal vesicle (behind bladder ) Seminal vesicle (behind bladder ) Urinary bladder Urinary bladder Prostate gland Prostate gland Bulbourethral gland Bulbourethral gland Urethra Urethra Erectile tissue Erectile tissue Scrotum Scrotum Vas deferens Vas deferens Epididymis Epididymis Glans penis Glans penis Testis Testis Male reproductive system
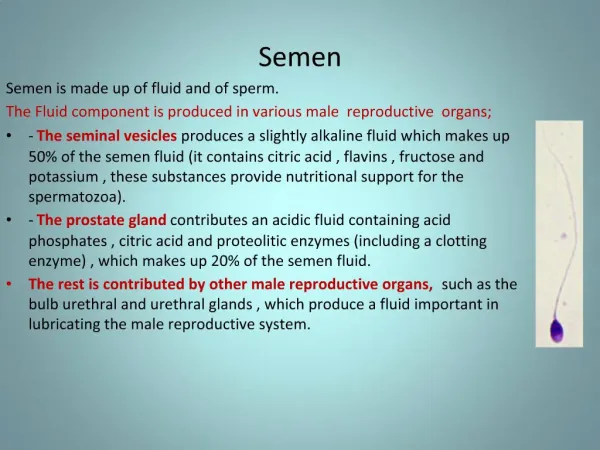
Accessory glands dysfunction 1) Seminal vesicles dysfunction : • Low volume • Decreased PH • Decreased fructose concentration 2) Prostate dysfunction : • Delayed liquefaction • Increased viscosity • Increased PH • Decreased zinc concentration
Spermatogenesis • Begins at puberty and continues throughout adult life of a male. • Sperm are produced within the seminiferous tubules. • Sertoli cells (nurse cells) feed and protect from a blood-testis barrier developing sperms. • Primordial germ cells differentiate into spermatogonia (diploid cells). • Spermatogonia during mitosis division become two primary spermatocyts.
Spermatogenesis • Each primary spermatocytes (diploid cells ) through meiosis I produce two secondary spermatocytes (haploid cells). • Each secondary spermatocytes during meiosis II divides to produced two spermatid (haploid cells with 23 chromosomes). • As a result of the two meiotic divisions, each primary spermatocyte produces fourspermatids.
Spermiogenesis • Changes that transform spermatids into sperm : 1) Chromatin condensation 2) Flagellum formation 3) Acrosome cap development 4) Discarding excess cytoplasm • Sperms transported to the epididymis (caput corpus caudal ) here they are stored. • Spermatogenesis takes 64 days in the human.
Examinations of human semen 1)Standard procedures Sample collection & delivery Initial microscopic & macroscopic examinations Anti-sperm antibody test (IBT & MAR test) 2) Optional tests Indices of multiple defect (TZI & SDI ) HOS test Semen culture CASA Biochemical assay (fructose, zinc) 3)Research tests Sperm function tests ROS Acrosome reaction CASA morphology
Sample collection & Delivery 1) Two samples 7days……3weeks 2) Sexual abstinence 2days……7days 3) Adequate collection • masturbation • non toxic glass or plastic container • no condoms • no lubricants • complete (important) 4) Adequate lab delivery ≤1 hour post collection 5) Adequate temperature 20 0C – 40 0C
Sample collection • Long sexual abstinence (Levitas et al. 2005) & (Pellestor et al.1994) • Increase sperm concentration • Increase volume • Decrease motility • Decrease normal morphology • Loss of the first part of the ejaculate : • Increase PH • Decrease sperm concentration • Delay liquefy • Loss of the second part of the ejaculate : • Decrease PH • Decrease volume • Increase sperm concentration • Lack of coagulum formation
Sample collectionat clinicorat home, which‼? Elzanaty & Malm, 2007 OBJECTIVE: Comparison of sperm parameters in samples collected by masturbation at clinic and at home. at a clinic (n = 273) PATIENTS 379 men at a home (n = 106) RESULTS : 1) Sperm concentration, total sperm count & rapid progressive motility were statistically significantly higher at home-collected samples. 2)Semen volume, normal morphology, PSA, Zinc & fructose did not differ significantly between groups. CONCLUSION :Superior semen quality in samples collected by masturbation at home compared with at a clinic. this should be taken into consideration in infertility investigation.
Semen collection methods 1) Masturbation 2) Coitus interruptus : • Loss of first portion of the ejaculate • Cellular & bacteriological contamination • The acid PH of the vaginal fluid 3) Semen collection in sexual dysfunction • Vibrator • Electro ejaculator (E.E) • Sperm retrieval methods: • PESA (Precutaneous Epididymal Sperm Aspiration) • MESA (Microsurgical Epididymal Sperm Aspiration) • TESE (TEsticular Sperm Extraction) MESA PESA
Initial examinations 1) Macroscopic : • Liquefaction • Appearance • Viscosity • PH • Volume 2) Microscopic : • Sperm motility • Sperm viability • Sperm concentration • Sperm morphology • Cellular elements other than sperm
Macroscopic examinations 1) Liquefaction time • Definition : the change from the coagulated to liquid. • Principl : proteolysis semenogelin by PSA • Normal : within 60 minutesbromelain(1g/l) • Abnormal : >60 minutes after ejaculation alpha amylase chymotripsin(150 USP/ml) 2) Appearance Normal: homogenous & grey-opalescent • Abnormal: • Opaque (debris or WBC) • Red −Brown (RBC) • Yellow (jaundice or taking vitamins) • Clear (poor sperm quantity)
Macroscopic examinations- continued 3) Viscosity (consistency) • Semen viscosity refers to the fluid nature • ↑ Viscosity = ↓ sperm motility • Normal: ≤ 2 cm thread 4) PH • Normal = 7.2 or more • PH is important because sperm die at PH < 6 • Routine measurement of PH is not necessary.
Macroscopic examinations- continued 5) Volume Low volume (hypospermia) :< 0.5ml • Seminal vesicle dysfunction or agenesis • Ejaculatory ducts obstruction • Retrograde ejaculation • Incomplete collection • High volume (hyperspermia) : > 6ml • Long periods of sexual abstinence • Over production of accessory glands • No ejaculate (Aspermia): • Surgery • Retrograde ejaculation
Assessment of motility Microscopic examinations • CASA( Computer- Aided/Assisted Sperm Analysis ) Systematic (manual method) : Grade a → rapid progressive motility ( ≥25 µm/s at 37 0C ) Grade b → slow progressive motility ( 5-25µm/s at 37 0C) Grade c → non progressive motility (<5 µm/s at 37 0C) Grade d → immotility • Asthenozoospermia: • Sperm structure defects • Prolonged abstinence periods • Varicocele • Anti-sperm antibody Cartagena's syndrome • Necrozoospermia : all sperms are dead Cilia immotile syndrome
Viability Microscopic examinations- continued • Distinguish live non motile sperm from dead. • Indication > 50% immotile spermatozoa • Determined by : Eosin staining Eosin- nigrosine staining Hypo-osmotic swelling test (HOS test ) • Hoechst staining Live Dead Live Dead
Sperm concentration Microscopic examinations- continued • Sperm concentration = number of sperm per ml of semen. • Azoospermia (no sperm in the ejaculate) • Obstruction • Hormonal insufficiency • Congenital Klinefelter's syndrome • Oligozoospermia ( <20 million sperm/ml ) • Procedural causes • Varicocele • Retrograd ejaculation • Polyzoospermai ( >250 million sperm/ml ) • Long sexual abstinence Improved neubauer Makler counting chamber
Assessment of morphology Microscopic examinations- continued • Most confusing & time-consuming area of semen analysis • Smearing, air-drying, fixation,staining • Staining method : Papanicolaou stain→ method recommended Pap-quick stain Diff-quick stain→ rapid staining method Shorr stain Wright-gimsa stain
Structure of normal spermatozoa 1)Headnuclear region • Oval in shape • Length: 4-5 µm & Width: 2.5-3.5 µm • Length-to-width ratio: 1.5 to 1.75 µm • Acrosomal region: 40-70% head area • Contain nucleus (DNA) 2)Midpiecemetabolic region • Slender & Width<1 µm • Length: about 1.5 times the length of the head • Contain axoneme & mitochondria • Cytoplasmic droplets less than half the size of the normal head 3)Taillocomotor region • Straight, uniform, thinner than the midpiece, uncoiled • Length: approximately 45 µm
Classification of sperm morphology 1) Head defects Small Large Tapered Round Amorphous Vacuolated Pyriform 2) Neck & midpiece defects Bent Thin Thick Asymmetrical insertion 3) Tail defects Short Coiled Double 4) cytoplasmic droplet or excess residual cytoplasmic ( >1/3rd normal head )
Sperm morphology classification systems Normal reference range 1) Macleod>60% 2) WHO manual 2nd edition >50% 3) WHO manual 3rd edition>30% 4) Strict (menkveld & kruger ) / WHO manual 4th edition>14% 5) WHO manual 5th edition >4% 6) ASCP (American society clinical pathology ) >80%
Cellular elements other than spermatozoa Microscopic examinations- continued • Round cells : < 5x106/ml • Immature germ cells : • Spermatogenic cells : fever, radiation, cytotoxic drug • Prostatic cells • Epithelial cells • Leukocytes : • Leukocytospermia ( >1x106/ml ) • Pyospermia (high amount of WBC) • Produce ROS, motility, aggregation • Antibiotic treatment