Download
1 / 25
250 likes | 385 Views
Overview of Health Insurance Exchanges, Basic Health Program, and Dual Eligible Integration. September 14, 2011. Amy Tenhouse Director of Policy Department of Policy and Government Advocacy. Molina Principles for Healthcare Reform Design. Health Insurance Exchanges.

E N D
Overview of Health Insurance Exchanges, Basic Health Program, and Dual Eligible Integration September 14, 2011 Amy Tenhouse Director of Policy Department of Policy and Government Advocacy
Health Insurance Exchanges (HIX) • Clearinghouse that facilitates individual and small business purchase of health insurance. • Web-based system similar to Travelocity or Expedia • Required duties of the individual Exchange: • Enrollment and consumer assistance • Eligibility determinations for public programs and subsidies • Oversight of Qualified Health Plans • Administration of the Exchange • Must be self-sustaining by January 1, 2015
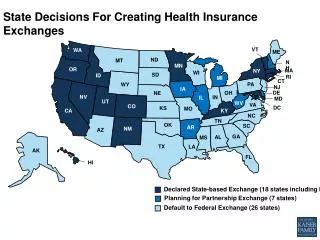
HIX State Efforts • HIX implementation is at various stages in Molina states:
Molina State Implementation of ACA: Exchange Activity in 2011 Enacted Legislation Legislation Vetoed Legislation Died No Legislation Introduced LegislationPending
Basic Health Program • Citizens and lawfully present immigrants who: • Are ineligible for Medicaid; • Have incomes at or below 200 percent of the federal poverty level (FPL); and • Lack affordable access to comprehensive employer-based coverage, as defined by the ACA. • Generally, there are two groups: • Individuals between 133 and 200 percent FPL • Lawfully present immigrants below 133 percent FPL who are ineligible for Medicaid (e.g., legalized within the last 5 years)
Basic Health Program • State contracts with health plans or provider networks • Competitive bids, multiple options for consumers (if possible) • BH-eligible people may not use the exchange • Premiums no more than what consumers would have paid in exchange • Out-of-pocket cost-sharing at or below certain levels • Statute: silver and gold actuarial value levels • HHS may say that OOP costs may not exceed levels in the exchange • At least minimum essential benefits • MLR at least 85% • Federal payments = 95% of federal subsidies if BH enrollees had been in the exchange
Reasons for Adopting Basic Health Program • Greater enrollment, more stable coverage as families stay together • BHP could smooth out the “cost–sharing shock” • Cost–sharing in the BHP would mitigate concerns about reduced preventive care and poorer outcomes for the low–income population • Provides states with more leverage in its direct purchases of coverage by allowing it to now buy on behalf of additional covered lives • A potential place to seamlessly absorb some of the children who will be impacted if CHIP funding is not extended after 2015
Reasons for Adopting Basic Health Program • States could invest unused funds into additional services including the ones that they fund with state $$ today. • Alternative for states looking to save previous expansions of Medicaid programs beyond minimal Federal levels or their locally developed programs for those above 133% of FPL • Supports safety net providers through higher reimbursements and retaining their patients • Medicaid/CHIP MCOs can easily extend services to BHP members based on their experience, cost, readiness, and knowledge of this population
Molina State Implementation of ACA: Basic Health Plan Activity in 2011 No Legislation Introduced Legislation Pending Existing Program prior to ACA
Basic Health Program State Efforts • Most Molina states have not begun to establish/consider BHP implementation. • California is exception. • Washington has existing program. • We have drafted BHP legislation that can be used in lobbying efforts.
Federal Medicare-Medicaid Coordination Office “Office of the Duals” • Focuses on improving Coordination between Medicare and Medicaid for dual eligibles • Will help to coordinate contracting and oversight functions by states and CMS • Focus in three major areas: • Program Alignment • Data and Analytics • Models and Demonstrations
Federal Medicare-Medicaid Coordination Office • To date, Coordination office initiatives include: • State demonstrations to integrate care for dual eligibles • Integrated care resource center available to all states • Initiative to align the Medicare and Medicaid Programs • Medicare data for dual eligibles for states • Demonstration program to test financial models to support state efforts integrate care for duals • Reducing preventable hospitalizations among nursing facility residents
Federal Medicare-Medicaid Coordination Office • State Demonstrations to Integrate Care for Duals: Integration Grants of up to $1 million each were awarded to 15 States to design new integrated care models. • Grants awarded to four Molina Healthcare states: CA, MI, WA, WI
Financial Models to Support State Efforts to Integrate Care for Duals • CMS seeks to test two financial models to better align the financing of the Medicare and Medicaid Programs. • Capitated Model: A State, CMS, and a health plan enter into a three-way contract, and the plan receives a prospective blended payment to provide comprehensive, coordinated care. • Managed Fee-for-Service Model: A State and CMS enter into an agreement by which the State would be eligible to benefit from savings resulting from initiatives designed to improve quality and reduce costs for both Medicare and Medicaid. • State Medicaid Director Letter released on July 8, 2011 • Letter of Intent due to CMS on October 1, 2011 • Target implementation date is 2012