Download
1 / 69
690 likes | 716 Views
Learn to diagnose and manage common orthopaedic injuries, including shoulder, elbow, hip, and knee issues. Understand both nonoperative and surgical treatment options available.

E N D
Common Orthopaedic Injuries Lutul D. Farrow, MD University Medical Center Human Motion Institute Assistant Professor, Clinical Orthopaedic Surgery University of Arizona College of Medicine Department of Orthopaedic Surgery
Disclosure • I have nothing to disclose
Objectives • After this presentation, the participant should be able to: • Diagnose common orthopaedic injuries • Understand nonoperative management of these injuries • List basic surgical treatment options for these injuries
Introduction • MSK injuries are common • 40% of complaints to PCP • Affects ADL’s • Lost work/wages
Overview • The Breakdown • Shoulder • Elbow • Hip • Knee
The Shoulder Basics • Shoulder problems are simple • Three diagnoses • Impingement • Arthritis • Instability
The Shoulder • It gets simpler! • Less than 25 • Think instability • Over 40 years old • Impingement • Arthritis
The Shoulder • Impingement • Blanket term • Multiple pathologies • Tendinosis • Bursitis • Rotator cuff tears • Biceps tendinopathy
The Shoulder • Pain generators • AC joint • Bursa • Rotator cuff • Biceps tendon
The Shoulder • History • Pain – variable location • PAIN WITH OVERHEAD ACTIVITIES • +/- Trauma • Subjective weakness • Easily fatigued • NIGHT PAIN
The Shoulder • Exam • Palpation • Impingement tests • Strength tests • Cervical spine
The Shoulder • Nonoperative treatment • Activity modification • NSAID’s • Physical therapy • Injections
The Shoulder • Operative treatment • Rotator cuff • Decompression • Biceps • Distal Clavicle • Arthroscopy
The Shoulder • Instability • 45% of dislocations involve glenohumeral joint • 85% anterior • Incidence - 1.7% (anterior dislocation) • Male (78%) >> Female (22%) • Much Higher incidence in persons < 30 y.o.
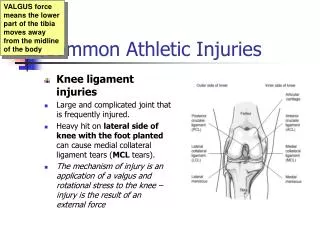
The Shoulder • Mechanism of Injury • Abducted, externally rotated arm • Humeral head driven anterior • Common in contact sports and overhead athletes • Hi-end athletes • Pathoanatomy • Torn capsule/ligaments • Torn Labrum • Variable bony injury • BEWARE RTC INJURY!!!!
The Shoulder • History • Traumatic Episode • Direction? • Red Herrings • Electrocution • Seizures • Physical Examination • Apprehension test • Rotator cuff
The Shoulder • Treatment • 1st timers • Rehab • Rehab • Rehab • Athletes and repeat offenders • Consider surgery
The Shoulder • Bottoni et al AJSM 2002 • Nonoperative: 75% recurrence • Arthroscopic stabilization: 11% recurrence • Kirkley, Miniaci et al Arthroscopy 1999 • Nonoperative: 47% • Arthroscopic stabilization: 15.9% (p < .03) • Porcellini et al Arthroscopy 2002 • Acute arthroscopic stabilization: • 92% stable at 2 year follow-up
The Shoulder • Sachs et al JBJS 2007 • 57% shoulders remained stable • 20% requested surgical stabilization • Conclusion • Need for surgery in the acute period cannot be predicted • Copers and Non-Copers • 60:40 Rule • 80% won’t need surgery!
The Shoulder • Surgical Repair
The Shoulder • Arthritis • Shoulder less commonly affected • Typically > 50 yo • Typically “post-traumatic” • Genetic predisposition
The Shoulder • Symptoms • Activity pain • ↓ ROM • Stiffness • Grinding/catching • Can mimic impingement
The Shoulder • Exam • Decreased ROM • Strength • Imaging • Plain films • MRI: little utility
The Shoulder • Arthroscopic debridement • Resurfacing • Hemiarthroplasty • Total arthroplasty • Reverse arthroplasty
The Elbow • Still keepin’ it simple • Bursitis • Epicondylitis • Ulnar nerve compression
The Elbow • Epicondylitis • Tennis elbow • Golfer’s elbow • Overuse injury • Poor ergonomics • Not true inflammation
The Elbow • Exam • TTP at or near tendinous insertion • Provocative tests
The Elbow • Nonoperative treatment • Physical therapy • Bracing • Activity modification • NSAIDs
The Elbow • Corticosteroid • Autologous blood • Platelet-Rich Plasma (PRP)
The Elbow • Corticosteroid injection • Point of maximum tenderness • Triamcinolone: 40 mg • 1% lidocaine: 6 cc • Peppering technique • Inject deep to tendon • Avoid fat atrophy • Avoids skin discoloration • AVOID SERIAL INJECTIONS!
Conservative Management • Corticosteroid therapy • Hay et al • BMJ 1999 • RCT: 164 patients • Corticosteroid injection, Naproxen, Placebo tabs • Take home • Corticosteroids are effective in the short term • At one year, most patients are better regardless of treatment modality
The Elbow • Autologous Blood • Platelet Rich Plasma
Conservative Management • Platelets • 1st on scene • α granules • PDGF • TGF – β • FGF • EGF • VEGF • Plasma • IGF-1 • HGF
Conservative Management • IGF • Accelerate healing in muscle/tendon • Menetry et al JBJS-Br 2000 • Kurtz et al AJSM 1999 • PDGF • Induces synthesis of other GF’s • Molloy et al Sports Med 2003 • ↑ biomech strength of healing tendons • Hildebrand et al AJSM 1998 • ↑ MCL strength (73%) at 12 days (murine) • Letson et al Clin Ortho 1994 • FGF • ↑ angiogenesis • Efthimiadou et al BJSM 2006
Conservative Management • 2 options for delivery • Autologous blood • Platelet-rich Plasma
Conservative Management • Autologous blood • Draw 2 – 5 cc of patient’s blood • Identical technique to corticosteroid • Point of maximal tenderness • Peppering technique
Conservative Management • Autologous blood • Suresh et al • BJSM 2006 • Dry needling medial epicondylitis • US-guided injection • Significant decrease VAS at 10 months • Significant decrease modified Nirschl scores • Resolution of Ultrasound findings • Take home: • Dry needling and US-guided autologous blood effective for treatment of refractory medial epicondylitis
Conservative Management • 2 options for delivery • Autologous blood • Platelet-rich Plasma
Conservative Management • PRP injected into injured tissue • Aim to enhance wound healing • Delivery of growth factors • Optimize healing environment • Active secretion w/in 10 min • 95% presynthesized w/in 1 hour • Marx JOMFS 2004 • Viable for 7 days • “Depot style”
Conservative Management • Platelet-rich Plasma • 6 to 8 x concentration • Mishra et al AJSM 2006 • Sample of whole blood • 55 mL • Citrate dextrose A • Anticoagulant • Prevents PLT activation • Activated with Ca2+ and Thrombin
Conservative Management • Classic technique • Required 2 “spins” • Commercially available separators • Single Spin • RBC’s • PRP • Platelet poor plasma (PPP)
Conservative Management • PRP Technique • Obtain 3 – 5 mL of PRP • Point of maximal tenderness • Peppering technique • Benefits • Minimal risk • Disadvantages • Cost: ~ $350 • Not covered by insurance (YET) • Large volume of blood
Conservative Management • Platelet-rich plasma • Mishra and Pavelko • AJSM 2006 • Refractory epicondylitis • 15 patients PRP • 5 patients bupivicaine • 3 of 5 bupivicaine patients sought surgery • Take home • PRP effective in refractory epicondylitis
The Hip • Most common players • Bursitis • Arthritis • Impingement
The Hip • Trochanteric bursitis • Inflammation of bursa • Gluteus minimus/medius • IT band • LLD
The Hip • History • Insidious versus acute • LATERAL hip pain • Sometimes buttock • Night pain • Can’t lay on hip • Injury – rarely • RA
The Hip • Examination • Point TTP • Ober’s test • LLD • Minimal pain with ROM • Resisted hip abduction • No xrays necessary • MRI if refractory
The Hip • Treatment • NSAID’s • Patches • Activity modification • PT • IT band stretching • Corticosteroids • Long needle? • Surgery • Very rare • IT band lengthening • Arthroscopic • Open