Download
1 / 16
160 likes | 430 Views
Accuracy of Radiology Trainee Major Trauma CT Reports. Dr Chris Bowles St George’s Hospital Ms IE Tribe, Dr S Ameli-Renani , Dr G Goh , Dr R Greenhalgh. Accuracy of Radiology Trainee Major Trauma CT Reports. Background Two cycle audit from April 2011 to September 2012.

E N D
Accuracy of Radiology Trainee Major Trauma CT Reports Dr Chris Bowles St George’s Hospital Ms IE Tribe, Dr S Ameli-Renani, Dr G Goh, Dr R Greenhalgh
Accuracy of Radiology Trainee Major Trauma CT Reports • Background • Two cycle audit from April 2011 to September 2012. • 1st cycle results • Intervention • 2nd cycle results • Questions
Accuracy of Radiology Trainee Major Trauma CT Reports • St George’s Hospital • Major Trauma Centre for Southwest London and Surrey Trauma Network • 120,000 patients/year through ED • Currently 120 Major Trauma patients per month • 1st Audit cycle- 1.98 Trauma CT/day • 2nd Audit cycle- 3.45 Trauma CT/day
Accuracy of Radiology Trainee Major Trauma CT Reports • Consultant Radiologist available on-site 8hrs/day. • 88-95% of Major Trauma CT initially reported by StR of varying grade. • Are we any good?
Accuracy of Radiology Trainee Major Trauma CT Reports • Previous studies have shown rates of consultant amendment of discrepancies ranging from 17-24% of scans, with major amendments from 5-10%. • Hillier JC et al. Trainee reporting of computed tomography examinations: do they make mistakes and does it matter? ClinRadiol2004;59:159–62Briggs, RH et al. • Provisional reporting of polytrauma CT by on-call radiology registrars. Is it safe? ClinRadiol2010;65:616-622 • Terreblanche OD et al. Should registrars be reporting after-hours CT scans? A calculation of error rate and the influencing factors in South Africa. ActaRadiol2012;53(1):61-8.
Cycle One • METHODS • Retrospective review of all Major Trauma CT scans for 6 month period April 2011-September 2011. • Classification of findings into • No acute traumatic injury • Minor Traumatic Injury • Major Traumatic Injury
Cycle One • Comparison with interval Consultant Final report • Note made of discrepancies • No impact • Minor Impact • Major Impact
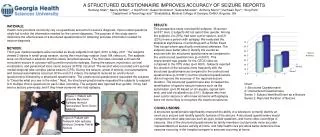
Cycle One • 358 scans performed. • 315 provisionally reported by StR (88%) • 207 (67%) had major or minor injuries on initial report. • 108 (33%) had no identifiable traumatic injury.
Cycle One • On Consultant review • 88 (43%) showed discrepancy. • 36 (17%) had no impact on management. • 49 (23%) had minor impact on management. • 3 (0.9%) had major impact on management.
Intervention • Oct 2011, CT Primary Assessment Proforma introduced.
Cycle Two • 6 month period April 2012-September 2012. • 622scans performed. • 591 provisionally reported by StR (95%) • 293 (37%) had major or minor injuries on initial report. • 382 (63%) had no identifiable traumatic injury.
Cycle Two • On Consultant review • 117 (19.8%) showed discrepancy. • 73 (12.4%) had no impact on management. • 39 (6.6%) had minor impact on management. • 5 (0.8%) had major impact on management.
Comparison • Between two cycles • Overall discrepancy rate dropped from 43% to 20%. • Discrepancy of no impact dropped from 17% to 12%. • Discrepancy of minor impact dropped from 23% to 7%. • Discrepancy of major impact stable between cycles (0.8%/0.9%)
Discussion • Significant post-intervention drop in overall discrepancy rate. • Major discrepancy rate was already low, didn’t change. • Minor discrepancy rate significantly improved. • Introduction of Primary Assessment Proforma gives ‘breathing room’ to reporting radiologist to allow comprehensive assessment.